
Substance Abuse Resources
Resources to better understand the nature of addiction and process of substance abuse treatment
Meetings & Programs
Twelve-Step Programs
| Organization: | Website: | Meeting Schedules: |
|---|---|---|
| Asheville Area Summary of 12-Step Meetings | Asheville Area AA Meetings | https://mountainx.com/support/ |
| Alcoholics Anonymous | www.aa.org | http://www.ashevilleaa.org/Meetings%20Map.html |
| Gamblers anonymous; | http://www.gamblersanonymous.org/ | Meetings within 100 miles of Asheville |
| Narcotics Anonymous | www.na.org | http://www.wncna.org/meetings/ |
| Information on Heroin Addiction | Information on Heroin Rehab | |
| Overeaters anonymous; | https://oa.org/ | Asheville OA Meetings |
| Sex addicts anonymous; | https://saa-recovery.org/ | http://www.orgsites.com/nc/saasheville/ |
| Sex & Love Addicts Anonymous; | https://slaafws.org | https://slaafws.org/meetings |
Support for Loved Ones
| Adult Children of Alcoholics; | www.adultchildren.org | Asheville area Adult Children Meetings |
| Al Anon, Al A teen; | www.al-anon.alateen.org | Asheville area Al-Anon Meetings |
| Co Dependents Anonymous; | coda.org/ | Asheville Area CODA Meetings |
| Narc Anon; | www.nar-anon.org | www.wncna.org/meetings/ |
Articles & Information
Medication Assisted Therapy
- Medications can make addiction treatment easier and more successful for the patient.
- Medically Assisted Treatment (MAT) involves the use of medications to not only help with the detox phase of treatment, but also to help patients have an easier time getting into recovery.
- Medications are available for abuse & addiction of all major drug classes;
- Alcohol
- Amphetamines
- Benzodiazepines & Barbiturates
- Cocaine
- Ecstasy
- Inhalants (huffing)
- Marijuana
- Methamphetamine
- Nicotine
- Opiates
- The best success rate for medication assisted therapy (MAT) is with opiates.
- There is no such thing as a medication to “cure” addiction.
- “Cure” means a one-time treatment producing permanent results
- Such as a “strept throat”
- “Control” means that if the treatment is used, the problem can be controlled.
- Diabetes, high blood pressure and others can be controlled but not cured.
- Treatment to control generally requires periodic monitoring and possible adjustments of dosage, medication and other factors.
- Various medications are used to treat addiction to specific substances
- There is no “one size fits all”
- Treatment is tailored to an individual patient’s needs
- “Dual Diagnosis” or “comorbid” conditions also need attention for successful treatment.
- Most folks use drugs to “feel better”
- Sometimes, people are self-treating various forms of mental illness that may have never been diagnosed, much less properly treated.
- “Cure” means a one-time treatment producing permanent results
- Numerous mental health issues must be addressed for proper addiction treatment;
- Anxiety
- Depression
- Bipolar Disorder (manic-depression)
- PTSD
- Psychological trauma
- Traumatic brain injury
- Many of these can successfully be treated and managed by an addiction-trained physician.
- Sometimes other help is needed
- Psychology
- Psychiatry
- Clergy
- Family therapy
- Although addiction can mimic every form of mental/emotional disease, treating the chemical imbalances caused by those conditions is crucial to attaining meaningful recovery for the patient.
- Ignoring these co-morbid/dual-diagnosis conditions does a great disservice to the patient!
- Sometimes other help is needed
Why are drugs addictive?
- The brain makes its own drugs! Drug Receptor location
- Endorphins & Enkephalins = Morphine/Heroin/Opioids Entire brain
- Anandamide = Cannabis/THC/Marijuana Sup. brainstem
- Acetyl choline = Nicotine Entire brain
- Dopamine = Cocaine, Amphetamine Mesocortex & Mesolimbic
- Gamma-HydroxyButyrate (GHB) = Alcohol, Benzodiazepines Modern & primitive brain areas
- Serotonin, Glutamate = Hallucinogens Parahippocampus & Cerebral cortex
- Drugs hijack the reward systems of the brain
- Drugs of abuse mimic the brains own neurotransmitters.
- They stimulate the brains receptors in the reward system causing dopamine release leading to the “artificial high”.
- Occasional use starts the Impulsive Cycle; “it feels good, let’s do it again!” (teaching the brain to anticipate reward).
- This leads to the Compulsive Cycle; repeated exposure leads toà craving toàbrain adaptation toàrepeated use…
- Neuroplasticity is the physiologic/anatomic term
- Neurobehavior change is the behavioral/mental health term
- Change in the number of receptors for a given drug or neurotransmitter in a specific area of the brain.
- Where & how do drugs work in the brain?
- Opiates
- Receptors are located diffusely throughout the brain
- Receptor Types
- Delta; pain relief, antidepressant, causes seizures & physical dependence, depresses breathing
- Kappa; pain relief, anti-seizure, depression, disassociation/hallucination, diuresis, dysphoria, miosis, neuroprotection, sedation, stress
- Mu1; pain relief, physical dependence
- Mu2; Respiratory depression, miosis, euphoria, constipation, physical dependence
- Nociception receptor (OLR1); anxiety, appetite, depression, development of tolerance to mu
- Zeta; tissue growth in embryonic development and regulation of cancer cell proliferation
- THC/Endocannabinoid system;
- Neocortex; higher cognitive functions/thought, integration of sensory information
- Cerebellum; motor control & coordination
- Has the largest number of endocannabinoid receptors in the brain.
- Hypothalamus; appetite, sleep cycle, sexual behavior, reaction to stress & hormonal levels (the neuroendocrine link)
- Basal Ganglia; motor control/coordination
- Ventral striatum; prediction and feeling of reward
- Hippocampus; memory, learning of facts, sequences & places
- Amygdala; anxiety, emotion, fear, paranoia
- Brain Stem & spinal cord; vomiting reflex, sensation of pain
- Opiates
- Acetyl choline/Nicotine system
- Two major types of receptors
- Nicotinic
- Muscarinic
- Receptor locations are throughout the brain;
- Thalamus, deep layers of the cerebral cortex, ventral tegmental area (VTA), medial habenula & substantia nigra (SN), pars compacta
- The a3 receptor is expressed strongly in the locus ceruleus, habenula & interpeduncular nucleus.
- Peripheral tissues also have a strong concentration of a3 in the autonomic and sensory ganglia.
- The a4 receptor is prevalent in the trigeminal ganglion
- Dopamine/Norepinephrine system;
- Mesolimbic; involved with ADD/ADHD, Addiction, Schizophrenia
- Mesocortical; ADHD, Addiction, Schizophrenia
- Nigrostriatal; Addiction, Chorea, Parkinson’s disease.
- Tuberoinfundibular; Hyperprolactinemia
- Gamma Hydroxy Butyrate/GABA/Glutamic system;
- Neuroinhibitory functions
- Main areas of activity;
- Frontal Cortex; memory, emotions, thought
- Cerebral cortex; thought, coordination
- Cerebellum; coordination
- Nucleus accumbens; Reward/addiction, works with dopamine and serotonin
- Amygdala; emotions, survival instinct, memory
- Hippocampus
- Two major types of receptors
Addiction is a DISEASE
- Our biology programs us to seek pleasure.
- Addiction is a disease of “self-will run riot”.
- Spiritual & social growth and maturation teach us to look out for the needs of others.
- This inherent conflict between “good for us vs. good for others” is a bit like “good vs. evil” and has plagued mankind since Adam & Eve.
- Addiction has multiple human axis’ or areas involved
- Biology
- Medicine is the art of “applied biology”
- Psychology
- Biology
- Sociology
- Spirituality
- The “BioPsychoSocialSpiritual” or BPSS.
- Addiction can happen in many forms;
- Substances (alcohol, drugs, food)
- Behaviors (gambling, love, codependence, sex)
- The American Society for Addiction Medicine (ASAM) states that genetics contribute 50% of this chronic brain disease.
- Genes load the gun, environmental exposure (using) pulls the trigger
- Nobody can choose their genetic makeup
- We couldn’t pick “better parents & genes”.
- Treatment provides education that helps people to understand and accept their genetic predisposition.
- Recovery consists of recognizing and understanding one’s genetic vulnerability.
- “Homeostasis” is the term used to refer t the tendency toward a relatively stable equilibrium between interdependent elements, especially as maintained by physiological processes.
- If something changes in one area, a corresponding change to balance the new system will happen elsewhere.
- Everyone has their own unique normal balance.
- Communication is essential to health.
- Our brain is constantly communicating
- Externally; sight, smell, taste, hearing, touch, voice
- Internally; our brain communicates through nerve cells; “neurons” that connect different areas of the brain.
Addiction is a PROGRESSIVE Disease
- It’s a disease of “yets”.
- “(Name your poor outcome/bottom) has not happened yet!”
- Even with periods of abstinence followed by later relapse, the depth of the relapse will be much worse than the status at their status at the earlier initiation of abstinence.
- Abstinence (not indulging in the substance/behavior) is NOT the same as recovery!
- Recovery is essentially the restoration of mental, emotional, spiritual & physical health.
- Addicts “use” to “feel better”.
- Imagine being able to “feel better” without the need to use!
- Addicts at some level will realize that they are “different” from “normal” people (normies).
- This difference is a gift!
- The gift of addiction means that we need to work harder for the spiritual connection than other “normies” seem to require.
- Sadly, in this culture, very few people recognize the need for that connection.
- Addicts do NOT have that luxury!
- When we actively pursue that connection with our higher power (whatever we conceive the higher power to be) we get incredible blessings or gifts for the extra effort required.
- Choosing to not pursue this connection is our death sentence!
- To an eternal death of our soul!
- Recovery is a process “time takes time”
- This is a process of growth
- Our spiritual self is always moving—either to greater recovery or backsliding to a relapse in addiction.
- There is no such thing as standing still!
- We must continually “work the program”
- The rewards of this are nothing short of AMAZING!
Acupuncture in Addiction (Acudetox)
- Acupuncture is a form of Chinese medicine that is over 5,000 years old.
- It’s still being used because it works!
- The theory behind acupuncture is that there is a flow of Chi (Qi), the vital life force in everybody, this energy of life flows through specific channels called meridians.
- Treatment can be done with beads, seeds, needles, needles with electrical charges applied and needles in which specific Chinese herbs are burned (moxibustion).
- There are 5 acupuncture points in the outer ear that are treated;
| Acudetox Point | Effects |
| ShenMen (Heavenly Gate) | Calms the spirit; decreases anxiety, insomnia & pain |
| Sympathetic | Calms the fight/flight response, sympathetic balancing |
| Kidney | Emotion & Fear |
| Liver | Detoxifies/unblocks stuck energy (emotional & physical), addresses the emotion of anger |
| Lung | Helps us “let go”, especially grief & sadness |
Spiritual Aspects of Addiction
- Addiction is a disease with much more than fascinating anatomy, physiology, pharmacology and behavioral aspects—it’s also a spiritual disease!
- Like any disease, it’s essential to evaluate and treat EVERY aspect of the disease before it can be subdued and controlled.
- There’s a difference between “religion” and “spirituality”
- Religion;
- the belief in and worship of a superhuman controlling power, especially a personal God or gods.
- “ideas about the relationship between science and religion”
- a particular system of faith and worship.
- a pursuit or interest to which someone ascribes supreme importance.
- Spirituality;
- A broad concept with room for many perspectives.
- Extra-corporal (without a body), non-physical.
- In general, it includes a sense of connection to something bigger than ourselves.
- It typically involves a search for meaning in life.
- As such, it is a universal human experience—something that touches us all.
- Religion;
- Transcendence; existence or experience beyond the normal or physical level.
- The concept of spirituality is different and much more simple than religion.
- Agnosticism or atheism does not need to be an obstacle to recovery from addict.
- All the 12-Step programs use the concept of a “higher power”, some people choose “God”, some don’t; and still get sober!
- “Higher Power” is whatever an individual addict chooses it to be for himself/herself.
- It does NOT need to be “God”.
- The USSR adopted the AA program referring to G O D as “group of drugs” despite their strongly professed atheistic state policy.
- All the 12-Step programs use the concept of a “higher power”, some people choose “God”, some don’t; and still get sober!
- Stanley Miller’s experiments demonstrated the possibility of creating organic compounds by applying energy to a “primordial stew”.
- Carl Sagan wrote that the odds against a specific human genome being assembled by chance as 1 in 102,000,000,000!
- It seems very unlikely that humanity came into existence solely by chance!
- Nature abhors a vacuum.
- There is no such thing as cold; it is simply the absence of heat.
- There is no such thing as darkness; it is simply the absence of light.
- Evil is the absence of good!
- We have AL seen evil at one time or another! Evil exists!
- Evil has a source; the Judeo-Christian and Islamic religions agree on the existence an evil spirit; Lucifer, Satan, Iblees, Jinn.
- The purpose of evil spirits (evil, fallen angels are known as demons) is to attack humanity and cause suffering.
- Thus, addiction may be thought of as a form of satanic attack!
- Occurring at the level of neuron membranes, receptors & neurotransmitters.
- And many other areas!
- Most religions believe in the existence of a soul, or spiritual force that each person possesses, something that lives beyond the physical death of the body—these souls are not demons, demons are “fallen angels” that numerous religions believe in.
- Souls are the spiritual component of individual human beings, not to be confused with the purely extra-corporal angelic or demonic beings.
- Since this is a disease with spiritual aspects to it, anything that improves the spiritual connectedness with the self-defined (and perceived) “higher power” will help the process of recovery.
- Addiction is associated with (some may say “caused by”) a disconnect with the “higher power”.
- Ancient cultures conjured up various deities to believe in to explain the unexplainable events of their reality.
- It’s been argued that this need to have a higher power of some sort is coded into our DNA, otherwise stated that…
- “We all have a God-shaped hole in our hearts” that we often try to fill with other “things”; substances of abuse, maladaptive behaviors, worldly objects that fail to fill the void that only a relationship with our higher power (God?) can fill.
- Who hasn’t experienced that undefined “feeling better” after going out of their way to help somebody in need?
- In the same manner, the “uncomfortable in my own skin” description often given by addicts resolves when they experience that deep joy from living in accordance with God’s plan for their life.
- Persons with addiction in early recovery are often encouraged to go out of their way to help another suffering addict when they are under stress, feeling bad and feel tempted to “pick up and use again” (relapse).
- Questions for personal reflection from the spiritual model:
- How do I evaluate my life in terms of my relationship with God or a “Higher Power”?
- How do I evaluate my life in terms of my own ultimate values and beliefs?
- Am I living in accordance with what I believe is important?
- Do I devote enough time reflecting upon my values and beliefs?
- The 12-Step programs help to cultivate and strengthen that connection.
- Initially, prayer (transmission to the higher power) may seem very “dry” and nonproductive.
- With continued prayer and meditation (reception from the higher power) and continued practice, that communication link to the higher power improves over time.
- The 12-Ste programs are associated with many short, pithy &profound sayings that convey basic concepts of the program that lead to success for those who “work the program” (not to be confused with “my” program—whatever one feels will work for them).
- “It’s a ‘me’ disease with a ‘we’ solution”.
- “Your best thinking got you here”.
- “Right actions lead to right thinking, feeling & acting”.
- “Suit up and show up, fake it ‘till you make it”.
- “It works if you work it, so work it ‘cause you’re worth it”!
- “He will do for us what we cannot do for ourselves”.
- Moral reconation therapy (MRT) is an evidenced-based addiction treatment aligned with this model. MR is not well known.
- Conation is an archaic psychological term referring to our capacity for conscious and deliberate decision making.
- This form of therapyis based on the outdated theory that addiction is simply a moral failing.
Clearly the science above shows MRT’s failings.
Recovery!
- The single most important predictor of successful long-term recovery is the motivation of the patient!
- The addict must put recovery ahead of everything else in their lives, if they start to falter, slow or stop aggressively working the program of recovery and putting it ahead of everything else in their life, they will lose.
- If they think their job & income is more important; that job & money will be lost with their next relapse.
- If they think a relationship with spouse, children, parents, siblings, friends is more important; those important people in your life will leave with relapse and failed recovery.
- Early recovery demands all your attention.
- The patient in the Intensive Care Unit (ICU) needs to concentrate on getting better.
- Early recovery is like being in the ICU, when an ICU patient improves they are transferred to a lower level of care in the hospital until eventually they are able to leave the hospital.
- Recovery is just like that; early, for at least the first year and until the 12 steps are worked under the guidance of a good sponsor, the addict should consider themselves to be in the “ICU” of recovery.
- Frequent 12-step meetings (90 meetings in 90 days is recommended as a bare minimum).
- Paying attention at those meetings, looking for the person who, every time they share, the recovering person feels that he/she “has what the addict badly wants and needs”.
- Frequent contact with other recovering people.
- Doing what is recommended by others in the meetings.
- Choosing a sponsor, at least a temporary sponsor initially.
- Following your sponsors advice completely and religiously, knowing full well that your sponsor is saving your life.
- Being totally honest (which will improve over time; the truth will come out like peeling the layers of an onion).
- You can’t handle the truth! (early in recovery it would overwhelm you, the truth comes out over time.
- Time takes time!
- The addict must put recovery ahead of everything else in their lives, if they start to falter, slow or stop aggressively working the program of recovery and putting it ahead of everything else in their life, they will lose.
- Later in recovery, you’ll learn to balance your life and include family, friends, career, money and integrate them all around your recovery program and spiritual development.
- There is also a lot to be said about having the addict take responsibility, financial and otherwise for their own recovery.
- Perhaps giving it to the family member or employee as a “gift” the first time can be considered, after that however…
- Responsibility includes “paying your way”; those who are constantly being “given everything” have no “skin in the game”!
- Recovery is there worthless to the mind of the addict.
- It didn’t cost them anything, so there is no value to it!
- The second most important point to make then, is that no matter how much you care for or love your addict, “tough love” may be the only thing that works.
- The addict MUST want to get better for themselves!
- They can not and will not get better for somebody else, no matter what they say.
- Addiction IS a disease of dishonesty and of…
- Self-will run riot—terminal selfishness!
- Recovery is a lot like sex; if you’re not having a great time, you’re doing something wrong!
- Mental
- It will take time for the distortions and fog to clear.
- Co-Morbid/dual-diagnosis conditions need to be diagnosed and treated properly in the early phases of treatment.
- The diagnosis and need for treatment with medications may change through the course of recovery.
- Addiction mimics every mental illness.
- A prudent therapist won’t give anybody a firm mental health diagnosis until at least a year of recovery (not abstinence) has passed.
- “Insanity”; repeating the same behavior, expecting a different outcome” (Albert Einstein).
- The more time in recovery that passes while working the full program of recovery, the more socially, morally balanced and integrated we become.
- “We will not regret the past nor wish to shut the door on it”.
- Emotional;
- Feelings are not facts and facts are not feelings.
- Addiction distorts and masks our emotions/feelings.
- Many addicts don’t fully understand what/how they are feeling at any given moment.
- Users typically use to “take the pain away”.
- This also numbers the normal, natural feelings that we all have.
- Feelings are neither good nor bad, they just are.
- Emotional growth appears to stop at the time of initial use of addictive substances (think of a 30-year-old person with emotional depth of a 15-year-old).
- Spiritual;
- Those who choose to cultivate a religious belief typically progress farther and faster in their recovery.
- They feel better sooner! (who wouldn’t want that?).
- Even the agnostic should consider this fact and reconsider their belief (or lack thereof) and become open-minded to change.
- Addiction is a “me” disease with a “we” solution.
- It’s a simple but not easy program.
- It’s only for those who want it, not for those who need it!
- Because of this, we cannot accomplish recovery alone, it requires the group dynamic.
- Physical;
- Addiction ravages the body, the exact organs damaged often depend on the substances & behaviors indulged in.
- Intra-venous drug abuse (IVDA) increases t risk of HIV & hepatitis (liver inflammation—often viral).
- Alcohol damages virtually every organ/system in the body.
- Tobacco damages the lining of airways, lungs & blood vessels.
- Complete cessation of abuse is crucial for physical recovery.
- Addiction ravages the body, the exact organs damaged often depend on the substances & behaviors indulged in.
- It’s not uncommon for miraculous physical recovery to occur among those who work the full recovery program
- Which means all 4 domains listed here.
- Many treatment centers ban smoking to stop all addictions in one treatment.
- This controversial step doesn’t happen in all treatment centers.
- True recovery integrates, coordinates and improves all the domains listed above.
- The 12-Step Program is the backbone of most recovery programs.
- Medications can be used to assist—but they only assist in the recovery process.
- Medications treat the biologic/medical aspect of BioPsychoSocialSpiritual (BPSS) of addiction.
- When dealing with addiction, a lethal, terminal, progressive disease, it’s best to use every tool available, all simultaneously.
- Jails, institutions and death are the ultimate (usually premature) outcome of this “cunning, baffling, powerful, ruthless & lethal” disease.
- Addiction is truly a terminal illness!
- Reasons for addiction continuation change over time;
- Early; “it feels good” (impulsion)
- Later; “it’s a habit” (compulsion)
- Finally; “I hate it and can’t stop because it hurts too much to try to stop”
- It’s important to understand in this disease model, that use/abuse of the drug/behavior is only a symptom of the underlying problem!
- Use/abuse/behavior is a coping mechanism to deal with the underlying dis-ease.
- Recovery entails fixing the problem at its root cause.
- “Recovery” entails working the program of recovery (verb).
- Addiction recovery has a few vitally important concepts;
- It’s a “me” disease with a “we” solution.
- It’s virtually impossible to get sober alone.
- With your distorted perceptions leading to faulty choices
- It’s a “simple” but not “easy” solution.
- It’s a simple program for complicated people.
- There’s nothing wrong with asking for help on a huge and difficult task
- Would you be reading this if you had gotten clean and sober by yourself?
- Repeating the same behavior while expecting a different outcome is insane!
- It’s a “me” disease with a “we” solution.
- Addiction recovery has a few vitally important concepts;
It WORKS IF YOU WORK IT; SO WORK IT ‘CAUSE YOU’RE WORTH IT!
How it Works
- Rarely have we seen a person fail who has thoroughly followed our path.
- Those who do not recover are people who cannot or will not completely give themselves to this simple program, usually men and women who are constitutionally incapable of being honest with themselves. There are such unfortunates. They are not at fault; they seem to have been born that way. They are naturally incapable of grasping and developing a manner of living which demands rigorous honesty. Their chances are less than average.
- There are those, too, who suffer from grave emotional and mental disorders, but many of them do recover if they have the capacity to be honest.
- Our stories disclose in a general way…
- What we used to be like.
- What happened, and…
- What we are like now.
- If you decided you want what we have and are willing to go to any length to get it—then you are ready to take certain steps.
- At some of these we balked.
- We thought we could find an easier, softer way.
- But we could not.
- With all the earnestness at our command, we beg of you to be fearless and thorough from the very start.
- Some of us have tried to hold on to our old ideas and the result was nil until we let go absolutely.
- Remember that we deal with alcohol—cunning, baffling, powerful, ruthless & lethal!
- Without help it is too much for us.
- But there is One who has all power—
- That One is God.
- May you find Him now!
- Half measures availed us nothing. We stood at the turning point.
- We asked His protection and care with complete abandon…
- Many of us exclaimed, “What an order! I can’t go through with it.’’
- Do not be discouraged.
- No one among us has been able to maintain anything like perfect adherence to these principles.
- We are not saints.
- The point is, that we are willing to grow along spiritual lines.
- The principles we have set down are guides to progress.
- We claim spiritual progress rather than spiritual perfection.
- Our description of the alcoholic, the chapter to the agnostic, and our personal adventures before and after make clear three pertinent ideas:
- That we were alcoholic and could not manage our own lives.
- That probably no human power could have relieved our alcoholism.
That God could and would if He were sought.
Sponsorship
- By going to meetings regularly, in part looking for that person, who, every time they share, you respect “what they have” and you “want what they have” (in terms of emotional sobriety, mental & emotional health).
- Asking that person to sponsor you is a great compliment to that person.
- You’re telling them how much you admire them and want to be like them!
- Work through the 12 steps as guided by your sponsor!
- The sponsor’s job is to guide the sponsee through the 12 steps of the program—not just to be there to listen to complaints about how tough life is!
- Your sponsor is not your bank, marriage counselor, therapist, doctor…
- This is not to be confused with “working my program”;
- “My” program; “my best thinking got me into this mess!”
- The program is what has worked for others (many worse than you).
- Stick with the winners, do what has proven to be successful!
- The 12-Step Program has the best documented and longest running success rate of any type of addiction recovery.
- Addiction is a disease of “self-will run riot”.
- It’s terminal selfishness, narcissism.
- “I may not be much, but I’m all I think about”.
- This s one of the most common denominators of addiction.
- It’s terminal selfishness, narcissism.
- Addiction is also a disease of dishonesty.
- To self and others.
- To self;
- DENIAL “Don’t Even kNow I Am Lying”.
- “If I can lie to myself so easily about this, I can certainly lie to others!”
- About having the disease;
- “I can stop anytime I want”.
- But you haven’t.
- Yet.
- To self;
- To self and others.
- Despite the numerous problems in your life, related, directly or indirectly to the illness.
- To others;
- Lies of Omission (leaving out pertinent information)
- Lies of Commission (active deceit)
- Hiding
- Your stash
- Amount of abuse
- Frequency of abuse
- Minimizing the amount used
Denial about outcomes related to abuse.
12 Step Program Pillars
- Self; we alone are responsible for our actions.
- Society; fellowship, we stand together and strive to interact with society at large.
- God (Higher Power); the source of the miracle of our recovery.
- Service; work to help each other.
- Freedom; the life-long process of healing & growth.
- Goodwill; toward others, to promote recovery.
- Unity; we work together
- Service; provided to each other.
- Recovery; growth, both collectively as a whole and individually.
- Circle; global reach.
Brain Biology
- Neurons have their own components.
- Dendrites receive information from other neurons.
- Axons transmit information to other neurons.
- Action Potential is the term used to describe the electrical transmission down the nerve, it’s a brief reversal of the normal (negative internal) voltage of the cell created by the passage of Na+ ions into the cell.
- The Synapse is a tiny gap separating neurons.
- Chemical neurotransmitters cross that gap to communicate to the next neuron.
- These neurotransmitters are stored in vesicles at the tip of the axon.
- An action potential (electrical depolarization/reversal of the normal negative internal voltage, propagates along the neuron triggering the release of neurotransmitter(s) into the synapse from the vesicle.
- Neurotransmitters are released into the synapse from the axon; a variety of possibilities occur after this step.
- Receptors for each different type of neurotransmitter are present on the “next neuron”.
- There are systems to recover (re-uptake) and recycle the neurotransmitter.
- Recovery sometimes happens on both (pre-synaptic &post-synaptic sides of the synapse).
- Drugs can have different effects;
- Mimic a neurotransmitter; “agonist”.
- Block a neurotransmitter; “antagonist” by occupying the receptor without causing the expected effect.
- This means that the proper neurotransmitter can’t occupy the receptor to trigger its normal function.
- Speed the reuptake/shorten the effect of the neurotransmitter.
- Slow the reuptake/lengthen the effect of the neurotransmitter.
- Binding is rarely, if ever permanent.
- “Affinity” measures the strength of the neurotransmitter/drug-to-receptor binding.
- High affinity means the bond is stronger and will last longer.
- This is not the same as “half-life” in the body.
- Which is generally determined by;
- Absorption through the gut for swallowed drugs, lungs/nose for smoked/snorted drugs, etc. into the blood stream.
- Distribution throughout the body.
- The rate of metabolism/chemical decomposition (breakdown) which generally occurs in the liver.
- Biotransformation to other metabolites which may or may not have effects on receptors/other parts of the body.
- Excretion usually through the kidneys, sometimes through stool, breathing, sweat.
- Receptors can also have different effects:
- They might trigger another action potential to depolarize/trigger the next neuron to send another action potential down it’s axon…
- They might open ion channels on the cell membrane locally to hyperpolarize and reduce the possibility of another action potential forming in the next neuron.
- Which is generally determined by;
- “Affinity” measures the strength of the neurotransmitter/drug-to-receptor binding.
- Chemical neurotransmitters cross that gap to communicate to the next neuron.
- Often numerous axons from different neurons in different parts of the brain will connect to a given “next neuron”; the end result will depend on the net effect on that “next neuron”.
- “It’s complicated!”
- This is the basis of how we think, remember, act, behave…
- Throw drugs into the mix and the overall effect is even more unpredictable…
- If that’s not complex enough…
- Genetics control differences in
- Every receptor
- For every different neurotransmitter
- Every neurotransmitter production system/capacity
- For each different neuron
- In each different part of the brain
- Every neurotransmitter reuptake/recycling system
- Both pre-synaptic &
- post-synaptic
- If it’s still not complex enough…
- Environment interacts with the genetics to influence the expression of our genes.
- Genotype is our genetic trait based on what genes we inherited from our parents.
- Allele is the term used to describe genotype differences such as
- Hair color
- Eye color
- Allele is the term used to describe genotype differences such as
- Genotype is our genetic trait based on what genes we inherited from our parents.
- Genetics control differences in
- Virtually everything else, including everything listed above
- Phenotype is the result of environmental interaction on our genetic trait
- VERY COMPLICATED INDEED!
- This nerve impulse transmission with multiple types of neurotransmitters is how thought & memory happen and all brain activity occurs.
- Drugs mimic neurotransmitters that are already present (generally in lower concentrations) in the brain.
- Use of drugs can thus alter behavior, perception, emotions/feelings, thoughts, memory, etc.
- Our endocrine system uses hormones to communicate and regulate the rest of our body.
- There is a neuroendocrine link as well;
- The Hypothalamus (Neural/brain) produces neurotransmitters affecting the Pituitary (Endocrine) Gland just beneath it which work together to produce
- Hormones (of the endocrine system) affect the rest of the body
- AND the brain!
- The pituitary is the “master” gland of the endocrine system.
- It regulates every other gland in the endocrine system.
- Examples of Drugs and the Neurotransmitter changes that they affect
- Hormones (of the endocrine system) affect the rest of the body
- The Hypothalamus (Neural/brain) produces neurotransmitters affecting the Pituitary (Endocrine) Gland just beneath it which work together to produce
- There is a neuroendocrine link as well;
| Drug | Neurotransmitters affected | ||
| Alcohol | Dopamine | GABA | Glutamate |
| Amphetamines | Dopamine | ||
| Benzo & Barb | Dopamine | GABA | Glutamate |
| Cocaine | Dopamine | ||
| Ecstasy | Dopamine | Serotonin | |
| Marijuana | Dopamine | Endocannabinoids | |
| Methamphetamine | Dopamine | ||
| Nicotine | Dopamine 2’ to | Acetyl Choline | |
| Opiates | Dopamine | Opiate | GABA |
- Note that dopamine is the common denominator for all addictive substances and activities.
iii. Dopamine is the “feel good” neurotransmitter!
Neurotransmitters; Drugs that Mimic them, Neurologic & Behavioral Effects
Neuroplasticity
- Drugs work on specific receptors
- “Neurons that fire together, wire together (form stronger linkages)”.
- There are many different types of neurotransmitters which have different type of effects
- Glutamate is generally excitatory
- Glutamine is generally inhibitory
- Gamma-Amino Butyric Acid (GABA) tends to calm/inhibit
- Serotonin also inhibits
- Norepinephrine is excitatory
- Dopamine is known as the “feel good” neurotransmitter
- Prolactin is the “in love” neurotransmitter
- Endorphins are mimicked by morphine and other opiates; they are naturally present in the body to relieve pain and other brain functions.
- Many other neurotransmitters exist; we still don’t know all of them!
- When there is an excess amount of activity of a neurotransmitter/drug activity (as in addiction/routine heavy use), the brain can respond by increasing the number of chemical receptors (E.g. On the “next” neuron) so that the excess amount of drug/neurotransmitter will have receptors to occupy while leaving some receptors empty to restore the “normal tone” of the brain in the presence of that excessive amount of drug/neurotransmitter.
- This is a natural compensatory “homeostatic” mechanism.
- This causes “tolerance”; the situation where the same dose of the drug has less of an effect such that more drug is needed to maintain the desired effect
- The opposite condition also occurs. If one has been a heavy user and suddenly stops, symptoms of drug withdrawal happen.
- At the cell membrane, what is happening is that there are now many empty, unoccupied receptors on the “next” neuron.
- This alters the normal function of that neuron
- Under conditions in which it would normally fire, or trigger an electrical impulse, it may remain silent, or under conditions in which it would normally be quiet, it may start sending false impulses.
- The withdrawal symptoms are specific to each various type of drug used.
- At the cell membrane, what is happening is that there are now many empty, unoccupied receptors on the “next” neuron.
- Detoxification;
- Withdrawal is never a pleasant process!
- It can kill as well!
- A brief review is in order;
- Alcohol withdrawal; can be lethal—needs to be done under medical supervision!
- Amphetamine withdrawal symptoms; sleepy, tired, irritable
- Barbiturate withdrawal; can be lethal—needs to be done under medical supervision!
- Benzodiazepine withdrawal; can be lethal—needs to be done under medical supervision!
- Cocaine withdrawal; irritability & fatigue.
- Marijuana; no significant withdrawal syndrome to worry about. The drug is stored in fat and slowly leaches out over time as an “auto-detox”.
- Opiate withdrawal; “dancing with the cold turkey”. Shakes, sweats, nausea/vomiting/diarrhea (NVD), tremors, yawning…
- You may feel like you would have to get better to die, and wish you would die, but you won’t.
8. Neuroplasticity is the term that describes both situations above, to many or too few receptors for the given condition—this is how the brain adapts to try to maintain homeostasis—a desirable steady state or “normalcy” of sorts.
Addiction Brain Regions Functions Neurotransmitters Input and Projection
Buprenorphine
Buprenorphine (Bup) effects;
- Consider different-colored padlocks (Delta, Kappa, Mu1, Mu2, Nociception, Zeta.
- Agonist agents fit into the lock, turn and open (activate) the lock
- Antagonist fits into the lock but won’t turn/open/activate the lock.
- This prevents any other molecule from engaging the receptor—blocking it’s effect
- BUP is a mixed agonist/antagonist;
- Partial agonist/antagonist at Mu1àPain relief
- Antagonist of Kappa
- Mixed effects on other receptor subtypes
- Norbuprenorphine is a metabolite of BUP
- Norbuprenorphine also has psychotropic properties
- Blocks the Mu2 receptoràno euphoria (“high”); it BLOCKS getting “high”
- 8 mg sl BUPà86% receptor blockade in opiate tolerate/dependent users
- 16 mg sl BUPà94% blockade
- 24 mg sl BUPà97% blockade
- The brain can tell the difference between 8 & 16 mg (86%-94%, or 8% receptor blockade)
- The brain cannot tell the difference between 16 mg & 24 mg (94%-97%, or 3% receptor blockade)
- However, 24 mg can be used short-term for acute pain syndromes if needed (Eg. After surgery)
- Remember, it blocks the euphoric effect
- “They sure don’t make heroin like they used to!”
- Prevents/relieves craving
- Stops pain; it’s used in open-heart surgery for pain control!
- Receptor half-life of 30 hours;
- Plasma half-life is 3-5 hours; high affinity means the receptor half-life is much longer.
- After 16 mg dose, in 30 hours, 8 mg still working…
- 30 more hours and 4 mg is still working and so on…
- Strong affinity for the mu-2 opiate receptor.
- The BUP-Receptor bond at the Mu-2 receptor is >500 times stronger than the receptors affinity for morphine.
- This means it takes a much longer time for it to randomly bounce off the receptor than morphine or heroin would.
- It should be noted that molecules and atoms “bounce around”; they have energy and will eventually leave the receptor, the stronger the affinity the molecule has for the receptor, the longer it will stay on the receptor.
- This explains why having used BUP will ruin attempts to get high by using heroin for more than a day after the last full therapeutic use of BUP.
- Transition from Methadone (MTD);
- This deserves special mention & review.
- Many “methadone clinics” put their patients on high doses of MTD whether they need it or not to control their addiction and/or pain.
- The best way to convert a patient from MTD to BUP is to start when the patient is down to 30 mg MTD/day.
- The patient may need to be slowly titrated down to this level, which may takes weeks.
- MTD has a prolonged and variable half-life of 8-60 hours
- It’s metabolized in the liver by the CytochromeP-450 CYP-3A4
- BUP is metabolized by the same liver enzymes.
- Converting patients from daily MTD doses >30 mg is possible but the patient will be uncomfortable—this is unavoidable.
- Due to the long half-life of MTD in the body, it must be stopped for 2 days before BUP can be initiated, even then, there will probably be opiate withdrawal symptoms.
- Medications are prescribed to ease the withdrawal symptoms.
- BUP treatment should be started when the patient is in early/mild opiate withdrawal.
- Starting this medication while the patient has high levels of other opiates (“pain pills”, heroin, MTD) can trigger opiate withdrawal/“cold turkey” symptoms.
- BUP is not absorbed in the gut, it works well transmucosally (across moist surfaces such as the inside of the mouth).
- Dissolve it in the mouth
- Saliva, once swallowed will waste the drug
- Repeatedly spread the saliva with the drug around the inside of the mouth—it’s absorbed on the inside surfaces of the mouth; cheeks, tongue, under the tongue, gums, etc.
- Try to keep the drug containing saliva in the mouth for 15 minutes
- Do not smoke cigarettes or anything else before taking the medication and for as long as possible after the medication
- Avoid brushing teeth before medicating and for as long as possible after medicating—some toothpastes contain astringents which can lessen absorption of the drug
- Forms;
| Subutex | Suboxone Tab | Suboxone Film | Zubsolv | Bunavail | |
| Dose | 8 mg | 8 mg/2 mg | 8 mg/2 mg | 5.7/1.4 | 4.2/0.7 |
| Retail Cost $ | $4.50 | $7.73 | $7.83 | $9-11.00 | $7.89 |
| Abuse Potential | NNNN | NNNN | NNNN | NNN | NN |
| Street Value $ | $25-40 | $20-25 | $15-20 | $20.00 | $15.00 |
| Discount | NA | NA | With card save $75/month for 90 films/year | First week free | Save up to $225/month or 90 films/year |
| Medicaid | Preferred |
- Naloxone is a rapid-acting opiate antagonist (blocker) that reverses/stops the effect of all opiates.
- Naloxone blocks ALL opiate activity
- This is especially useful in overdose when breathing stops
- It can restore breathing, blood pressure, etc.
- Evzio Autoinjector; (~$3,742.90 per dose)
- Narcan; (~$65.70 per dose)
Diagnostic Criteria for Addiction
- Tolerance, as defined by either of the following:
- A need for markedly increased amounts of the substance to achieve intoxication or the desired effect or
- Markedly diminished effect with continued use of the same amount of the substance
- Withdrawal, as manifested by either of the following:
- The characteristic withdrawal syndrome for the substance or
- The same (or closely related) substance is taken to relieve or avoid withdrawal symptoms.
- The substance is often taken in larger amounts or over a longer period than intended (largely due to tolerance (a.).
- There is a persistent desire or unsuccessful efforts to cut down or control substance use.
- A great deal of time is spent in activities necessary to obtain the substance (such as visiting multiple doctors or driving long distances), use the substance (for example, chain-smoking), or recover from its effects.
- Important social, occupational, or recreational activities are given up or reduced because of substance use.
- The substance use is continued despite knowledge of having a persistent physical or psychological problem that is likely to have been caused or exacerbated by the substance (for example, current cocaine use despite recognition of cocaine-induced depression or continued abuse despite recognition that an ulcer was made worse by illicit consumption).
- Legal problems related to abuse.
- Medical problems related to abuse.
Addiction Prevalence
- 41% Incidence of any use over the lifetime of any illicit drug.
- Admittedly 41% can include one-time use of a substance which is hardly addiction
- 5% incidence of any use of illicit drug in the past month.
- Monthly use is much more regular use than use in the past year or lifetime.
- This information is obtained from surveys.
- Survey data often underestimates actual use
- Minimizing use is common among addicts.
- Minimizing is a form of denial.
- Considering the above, it’s quite possible that up to 10% of the population may have a problem with substance abuse (excluding tobacco)!
- Incidence of use/abuse of drug within the US (total population age>12 years):
| Substance use/abuse 2015 US Pop. | Lifetime 2015 % | Past Month % | Past Year % |
| Any Illicit Drug | 41 | 8.5 | 15 |
| Alcohol abuse | *? | ? | 13.8 |
| Amphetamines | ? | 0.5 | 2 |
| Benzodiazepines (& Barbiturates) | ? | 0.7 | 2 |
| Cocaine | 15 | 0.5 | 2 |
| Ecstasy | 5.7 | 0.2 | 0.7 |
| Hallucinogens | 12.7 | 0.4 | 1.5 |
| Heroin | 16 | 0.1 | 0.2 |
| Inhalants (inhaling organic solvents) | 8 | 0.2 | 0.5 |
| Ketamine | ? | ? | 0.4 |
| Marijuana | 24 | 7 | 11.3 |
| Methamphetamine | 4.5 | 2 | 5 |
| Opiates (other than heroin/ “pain pills” | ? | 0.1 | 3.9 |
| * ?; Data conflicting or unavailable.
— The lack of sums adding to the total illicit use reflects abuse of more than one substance by survey participants. = This table does not include ALL drugs of abuse, only those most commonly used and tracked by researchers. |
|||
- When one considers the scale of the use of psychoactive substances currently in the US and considers that addiction is often characterized by the abuse of multiple substances, there is a clear cause for concern.
- Abuse of illicit substances costs the US $193,000,000,000 annually
Total substance abuse costs including alcohol and tobacco are >$700 billion/year.
Addiction Distorts Perceptions
- Not only when high/stoned/abusing the drug, but even before the drug has EVER been tried.
- Addicts/alcoholics “see things differently” and react differently.
- The first use of the substance seems to “let the evil genie out of the bottle” accelerating the course of the disease of addiction.
- Addicts use these distorted perceptions to make decisions.
- Their choices often lead to less than desirable results.
- Emotional growth is thought to stop at the age of first use of addicting agents.
- This is even more pronounced with drugs such as THC that affect the pre-fontal cortex where judgement and impulsivity control reside.
- In short, addicts end up with changes in the brain that are best described as a form of brain damage.
- “Two heads are better than one”; “collective brain power” can be a good defense, but where do you get the heads that can understand and reason with the addicted/afflicted?
- The “12-Step Meetings”
- Look for the group members with long-term sobriety!
- Get there well before the meeting starts for the informal “meeting before the meeting”
- Stay afterwards for the “meeting after the meeting”
- The folks who are going to meetings now are the same folks who used to be the “life of the party”
- They INSIST on having a good time
- They love to laugh and kid around
- They cannot keep their own gift of recovery without giving it away to newcomers whenever the opportunity arises
- Newcomers are helping them by showing up at meetings!
- They will insist that the above is true—they really mean it!
- Even if you’re not welcome anywhere else, they will welcome you warmly.
Psychological Aspects of Addiction
- It’s important to understand the difference between Psychiatry and Psychology:
- Psychiatrists are physicians (MD or DO), they prescribe medications to correct abnormal brain chemistry as reviewed above, they tend to place emphasis on neurochemical modifications of one’s emotional and mental problems and state.
- Psychologists generally have a doctorate in what can be considered “talk therapy” which involves discussion with the patient, diagnosis forming and a variety of different types of talk therapy to help the patient come to an understanding of differing perspectives, ideas, beliefs & ultimately feelings and behaviors.
- Psychological theories on why addiction happens;
- Addicts may engage in harmful behaviors because of concurrent mental illness.
- They may learn unhealthy behavior in response to their environment.
- Thoughts and believes create feelings….
- Which in turn determine behavior.
- If thoughts, beliefs & feelings are unrealistic/dysfunctional, behavior may be affected.
- Psychologists assume these theories apply in some way to addiction.
- People with these disorders might include cognitive difficulties, mood disturbances and other mental illnesses.
- Addiction & other mental health disorders commonly occur together (co-morbidity).
- Half of the people seeking addiction treatment will have another significant mental health disorder (Miller, Forchimes & Sweben, 2011).
- Many who suffer from addiction have attempted to “self-treat” their mental illnesses with available psychoactive substances (drugs) to ease their suffering.
- Examples of emotional/mental disorders commonly comorbid with addiction include;
- ADD/ADHD
- Anxiety
- Bipolar disorder
- Depression
- PTSD
- Trauma
- Addictive personality;
- A set of personality traits that predispose an individual to developing addictions.
- This hypothesis states that there are common elements among people with varying addictions that relate to personality traits.
- There are several distinct personality disorders listed in the Diagnosis and Statistical Manual Edition 5 (DSM-5, the basic handbook of psychiatry and psychology that codifies all emotional/mental health disorders).
- Review of the Personality Disorders in the DSM-5R reveals the absence of an “addictive personality disorder”.
- There are basic/informal/not coded personality traits associated with addiction;
- Denial of obvious problems
- Problems with emotional regulation.
- Problems with impulse regulation.
- Psychotherapy attempts to identify and resolve underlying psychological disorders.
- Self-realizations and help from a qualified therapist can help uncover some of these issues.
- The “therapeutic relationship” of the patient with the therapist is critical to ensure enough trust is present that difficult issues can be explored.
- A set of personality traits that predispose an individual to developing addictions.
- Absolute honesty and diligence is required for success in any such form of therapy.
- Locus of control;
- Recognition and acceptance of personal responsibility for problems and their solutions bring to the surface deeper underlying issues.
- Do we see ourselves as internally directed, responsible for our own actions or…
- Externally directed; “things just happen because they happen”, we don’ have much responsibility for the major events of our lives “Fate or “Karma”-driven.
- A brief online test can help determine which locus of control you believe in.
- Nobody is entirely internally or externally directed, generally though, we all have a predominant belief in one vs. the other.
- Theories regarding responsibility for addiction;
- The “Medical Model”: People are not responsible for creating or solving their own problems.
- The “Compensatory Model”: People are not responsible for creating, but are responsible for solving their own problems.
- The “Moral Model”: People are responsible for creating and solving their own problems.
- The “Enlightenment Model”: People are responsible for creating, but not solving their own problems.
- Recognition and acceptance of personal responsibility for problems and their solutions bring to the surface deeper underlying issues.
- What’s the best way to make sense of all of this?
- Since we’ve established the genetic/biologic/medical basis of addiction and the fact that none of us can choose our parents, it seems that the compensatory model fits…
- People are responsible for solving, but not creating, their own problems, thus the compensatory model…
- Yet, who among us hasn’t behaved in a manner that worsened our addiction, made poor choices, leaving us to consider other options. We’ve established the biological nature of the illness which makes the moral model less likely…
- Wouldn’t it be great if we were not solely responsible for fixing the mess that we’ve made of our lives?
- This line of thought leads us to an answer…
Effects of Addiction on Your Family
- Addiction has genetic underpinnings.
- If one parent is susceptible to addiction (whether they choose to “use” or not), there is a 50% chance that offspring will have the gene.
- If both parents carry the gene the chance of passing it on are closer to 100%
- The genetics of addiction probably involve numerous genes, are thus complex and not yet fully understood.
- A review of family history will often reveal members of the family tree who were alcoholic, addicted, suffered from emotional/mental disorders or died early.
- Suicide is often associated with addiction.
- Recall that mental health is a very new field of study, even a generation ago somebody may have been considered “not right in the head” or avoided if not outright shunned and not talked about in family discussions.
- Obviously, the addict’s behavior has wide-ranging effects on not only the immediate nuclear, but often on more extended family members as well.
- Many families with a presence of addiction attribute addictive behavior to “normal”
- “It’s the only behavior we’ve ever known”.
- Families and people are thought of to be “only as sick as their secrets”
- We learn at a tender young age that “there are certain things we just don’t talk about outside of our family”.
- This simply perpetuates the problem.
- Codependence can be considered as another aspect of addiction.
- It can also be considered as an addiction all to itself
- One is addicted to the addict that they are enmeshed with in their codependence.
- Family members enable the addict(s) to continue their behavior in many ways
- It can also be considered as an addiction all to itself
- “Calling in sick” for them when they’re unable to attend to their responsibilities due to effects of the substance/behavior or its withdrawal.
- Tolerating and hiding unacceptable behavior
- “Accepting unacceptable behavior makes it acceptable”.
- Divorce & failed relationships are often due directly or indirectly to addictive behaviors
- This may be frustration in dealing with the “ism” of alcoholism or “drugism”
- “…ism”= “I”, “Self” & “Me”
- “I’m not much but I’m all I think about”.
- Such behavior has its limits and is rarely tolerated forever.
12 Step Programs
- Addiction encompasses alcohol and other drugs that are abused.
- When attending an AA Meeting, it’s best to introduce yourself as an alcoholic
- At an NA meeting the term “addict” is generally preferable.
- A middle-of-the-road term; “I’m an alcoholic and drugs were part of my problem”.
- Crossing the wrong term for the meeting attended may result in grumbled comments from a member of the group
- We’re not in these meetings because we’re so healthy, we’re there because “we aren’t all ‘there’”!
- There are a variety of other 12-step meetings as well;
- Sex & Love Addicts Anonymous; https://slaafws.org.
- Sex addicts anonymous; https://saa-recovery.org/.
- Overeaters anonymous; https://oa.org/.
- Gamblers anonymous; http://www.gamblersanonymous.org/.
- Additionally, there are meetings for the loved ones of those addicted.
- These meetings usually end with “anon”
- Al Anon, Al A teen; http://www.al-anon.alateen.org/.
- Narc Anon; http://www.nar-anon.org.
- Adult Children of Alcoholics; http://www.adultchildren.org.
- Co Dependents Anonymous; http://coda.org/
- Co-dependence is the term used for those who have enabling behavior
- This is a form of behavior meant to be helpful, but in the long run is harmful for the addict.
- This can be thought of as another expression of addiction—that other person is hooked on the emotional state of the addict.
- An easy example would be a spouse calling in sick for the hung-over alcoholic so that he/she doesn’t get in trouble at work.
- The line between helpful and enabling is very thin and “moves” over time—it’s VERY helpful to have another person, ideally a sponsor in that program who is not emotionally invested in the addict help to navigate & determine the best course of action in various aspects of the disease of addiction and interactions with the beloved.
- These meetings usually end with “anon”
- These meetings for loved ones also have their own 12 steps, sponsors, etc. for the family to work with.
- When attending a 12-step meeting, there will be a “meeting before the meeting” and a “meeting after the meeting” where folks hang out and chat before and after the meeting.
- This is the IDEAL time to share what’s going on in the newcomer’s life!
- It’s great to discuss problems, concerns and plans to resolve the issues.
- Typically, the longer a person has been sober, the better their overall mental health is.
- It’s a good idea to attend meetings with as much “long-term sobriety” as possible.
- Some meetings can have hundreds of years of sobriety collectively in each meeting.
- 20 attendees with 5 years of sobriety each = 100 sober years.
- 5 attendees with 20 years of sobriety each = 100 sober years.
- Ideally the most long-term sobriety (i.e. “b”) is preferred.
- Often, there is more long-term sobriety in AA than in NA meetings.
- But at the same time, triggers to relapse will be different between the two programs.
- There will be differences between addictions to various substances/activities.
- It’s best to include the meeting best suited to any given person’s predominant addiction.
- Many folks will have multiple addictions.
- Cross-addiction refers to stopping use of one addiction only to pick up another.
- When an addict stops using a certain drug that does not mean that it’s OK to use other emotion/mind altering substances or behaviors.
- Cross-addicting to another substance or behavior is a very real danger.
- Even the opiate addict who hates alcohol can very easily become an alcoholic if they dabble in using alcohol occasionally
- Those addiction circuits in your brain are still there, dopamine, the “feel good” neurotransmitter is still the final common outcome neurotransmitter for all addictive substances and behaviors!
- As important as meetings and sponsorship are, there wouldn’t be much hope without the 12 Steps of the Recovery Program.
12 Promises & Rewards of Recovery
- Recovery is not about “not using”; it’s about having such a GREAT LIFE that you don’t WANT to use!
- Imagine being able to attain the peace of mind and relaxation that in the past required using/abusing substances/behaviors, but being able to do so without abusing and to live peacefully in that state!
- 12 Promises;
- We are going to know a new freedom & a new happiness
- We will not regret the past nor wish to shut the door on it.
- We will comprehend the word serenity.
- We will know peace.
- No matter how far down the scale we have done, we will see how our experience can benefit others.
- The feelings of uselessness and self-pity will disappear.
- We will lose interest in selfish things and gain interest in our fellows.
- Self-seeking will slip away.
- Our whole attitude and outlook on life will change.
- Fear of people and of economic insecurity will leave us.
- We will intuitively know how to handle situations which used to baffle us.
- We will suddenly realize that God is doing for us what we could not do for ourselves!
- 12 Rewards of Recovery;
- Hope instead of desperation.
- Faith instead of despair.
- Courage instead of fear.
- Peace of mind instead of confusion.
- Self-respect instead of self-contempt.
- Self-confidence instead of helplessness.
- The respect of others instead of their pity and contempt.
- A clean conscience instead of a sense of guilt.
- Real friendships instead of loneliness.
- A clean pattern of life instead of a purposeless existence
- The love and understanding of our families instead of their doubts and fears.
- The freedom of a happy life instead of the bondage of addictive obsession.
12 Steps
- Step 1; Weadmitted we were powerless over drugs/alcohol—that our lives had become unmanageable.
- We this is a “we” program, nobody can get straight alone, we’re in this together!
- Admitted became aware, realized, recognized & let it be known to others.
- Powerless lack of control or ability to influence.
- Drugs/Alcohol this is the only mention of substances/behaviors in any of the 12 steps
- The abuse is merely a symptom of our disease.
- Unmanageable we are unable to cope, uncontrolled.
- Step 2; Came to believe that a power greater than ourselves could restore us to sanity.
- Came
- Came to
- Came to believe
- A power; something supernatural—back to the spiritual—but let’s not call it “God”.
- That term drives people who need help away, let’s use another term.
- “Higher Power” admits to the possibility of something transcendent, even if it’s only a “group of drunks”.
- Restore to replace what was lost.
- Sanity the ability to think and behave in a normal and rational manner, sound mental health.
- A trained behavioral scientist in 12-Step meetings can make diagnosis of virtually every mental illness imaginable.
- These diseases are all treated differently with medication and type of therapy.
- Yet they ALL improve by working the 12-Step program.
- By the same measure, it’s impossible to diagnose with certainty any mental illness in the disease of addiction until at least a year of recovery has happened.
- Another miracle of the program
- Addiction can manifest as every known form of mental illness.
- Addiction amplifies and exaggerates these diseases as well.
- This is yet another example of the distortion caused by addiction.
- Step 3; Made a decision to turn our will and our lives over to the case of God as we understood Him.
- This is another key concept for recovery!
- Decision a choice that we freely make without coercion.
- Turn our will and our lives…
- This is HUGE; we’ve surrendered completely and given up trying to control our lives for ourselves.
- THIS is the ACCEPTANCE of God’s will in our life.
- The care of God/Higher Power understanding that we are under His/It’s care and that He/It has care and concern for us, wishes us well and that no matter how bad things seem to get, it will ultimately be in our best interest.
- In the 12-Step programs, we share our experience, strength and hope.
- We don’t give advice or direction
- My personal experience has been that my Higher Power (whom I choose to address as “God”) allows me to go through difficulties in life.
- Growth often involves pain!
- I come out of these difficulties as a much stronger and better person than before the situation.
- Faith is stronger after such a test.
- We can choose to violate the decision and try to run away from the lesson—but it will find us and probably be repeated a few more times in our lives to ensure that we truly learned that lesson.
- In the 12-Step programs, we share our experience, strength and hope.
- Since we’ve learned that addiction can mimic all known emotional & mental illness’, it can be useful to think of this as one of the many miracles provided by the Higher Power (whatever you conceive that to be, the one you agreed to the existence of in Step 2 above).
- Once we truly decide to turn ourselves over, the miracles of the promises begin.
- The miracles will continue so long as the program is practiced and shared with others!
- Step 4; Made a searching and fearless moral inventory of ourselves.
- This is the first “action step”, it involves pen & paper.
- It will take a lot of time, work, reflection and help from a good sponsor.
- Sometimes a good therapist may be helpful or required.
- This involves a thorough and complete moral inventory—the good and the bad.
- Not just what you did right or wrong, but why you did so.
- A good sponsor is essential for this step.
- This is about more than wrongdoing, it’s about the underlying reason for the wrongdoing.
- Without being completely thorough and honest, future relapse is likely.
- This will also form the basis for the 8th and 9th
- Step 5; Admitted to God, to ourselves, and to another human being the exact nature of our wrongs.
- God; it’s OK to use “Higher Power” if preferred.
- Another human being it’s essential to communicate this information, derived from Step 4 to another person.
- Often, but not necessarily your sponsor.
- Ideally/often, the other person (sponsor?) will share similar issues/experiences with the person doing the step (sponsee?).
- Not just what you did right or wrong, but why you did so.
- This is the first “action step”, it involves pen & paper.
- Exact nature involves not only the wrongdoing, but the underlying reason/motive behind it.
- Step 6; Were entirely ready to have God remove all these defects of character.
- The Higher Power from Steps #2 & #3 is the source of this healing, restoration to sanity and revocation of mental illness.
- The compulsion to drink may be lifted with Step #3, sometimes persisting longer, if so it may resolve after Step #6.
- Entirely ready means without reservations, no matter what may come.
- God (Higher Power) removes these defects, but only with our unreserved consent and cooperation.
- Defects/faults/failures
- Character our most basic moral character.
- Step 7; Humbly asked him to remove our shortcomings.
- “When you have nowhere else to turn, and are on your knees, turning to your Higher Power, you are at your strongest!”
- This is done with the humble realization that we have not been able to heal ourselves.
- Admitted that our issues have been shortcomings.
- Step 8; Made a list of all persons we had harmed and became willing to make amends to them all.
- After having done Step #4, with the realization of the harms done by our moral failings and faults, it’s now time to start contemplating being able to make appropriate amends and to whom.
- This also requires review with a good sponsor.
- It’s not about making amends, it’s about becoming ready and willing to do so.
- Made this is another action step.
- A list of all persons everybody and the list will include 2nd generation harms, we may have caused somebody to harm another due to the harm that we di to them.
- Become willing in part because of having done the 5th Step, willing to make amends to them all.
- Step 9; Made direct amends to such people wherever possible, except when to do so would injure them or others.
- Amend; make better, improve.
- The US Constitution has 27 amendments.
- None start with an apology!
- Imagine driving a huge railroad spike into the middle of an expensive polished mahogany conference table.
- An apology would entail removing the spike, leaving a large hole
- An amend is to fix the table in a matter satisfactory to the owner of the table.
- Except when to do so would involve injury to them or (especially) others.
- An example would be undiscovered infidelity.
- If the victimized spouse was ignorant of the wrongdoing, to expose it would cause that spouse pain.
- If there has truly been a change and future transgressions are quite unlikely, then there would be nothing positive to gain by exposing the prior error.
- The amends process is to heal you, not the other person.
- It releases you from a spiritual bondage/guilt toward that other person.
- Step 10; Continued to take personal inventory, and when we were wrong, promptly admitted it.
- Continued means that this is an ongoing process, often done at the end of each day, with a daily review/reflection, especially regarding any problems that may have occurred and how I responded.
- When we were wrong recognized when we had committed a transgression
- An example would be undiscovered infidelity.
- The US Constitution has 27 amendments.
- Amend; make better, improve.
- Promptly admitted it without delay and made amends as soon as possible.
- Step 11; Sought through prayer and meditation to improve our conscious contact with God as we understood Him, praying only for knowledge of His will for us and the power to carry that out.
- Sought we continue daily to pursue our Higher Power in Whom we’ve entrusted ourselves without reserve.
- Prayer & meditation
- Prayer can be thought of as our transmission upward, an upload of sorts, to our Higher Power.
- Meditation is our reception, or download from our Higher Power
- Improve our conscious contact acknowledges that we do have a conscious contact with our Higher Power; this is the essence of spirituality.
- As we understood Him remember, this is our own personal Higher Power.
- The same One we chose & defined for our self in our 2nd
- The same One we turned our lives over to.
- The same One we chose to heal us.
- The same One who removed our shortcomings, including our compulsion to use and Who gave us the gift of recovery!
- Knowledge of His will for us we are to pray only for that which He wants for us.
- We turned ourselves over to Him in Step #3. This reinforces that decision!
- We acknowledged that He alone knows what is best for us.
- And the power to carry that out.
- He alone gives us the power to do His will.
- He will provide us with the power to do His will.
- He is the “Miracle Department”.
- He has better plans for our life than we have for our life!
- Step 12; Having had a spiritual awakening as the result of these steps, we tried to carry this message to alcoholics and to practice these principles in all our affirs.
- Had
- We have already
- It’s a done deal!
- There is no more doubt about it being possible, it’s an established fact by now!
- Spiritual awakening
- Established and continued to enhance and maintain our relationship with
- The Transcendent
- My Higher Power (God?)
- While many agnostics enter the 12-Step programs, within 5 years, few of these folks continue to describe themselves as agnostic.
- Faith grows!
- Established and continued to enhance and maintain our relationship with
- Had
- Result of these steps
- Clearly, this is the outcome.
- Of all the work that we’ve done to date and…
- Our sacrifice of “self” to our Higher Power’s will
- Carry this message
- Carry;
- To maintain with me, myself and
- To convey to others.
- This message;
- The gift of recovery.
- Steps
- Meetings
- The gift of recovery.
- Carry;
- Sponsorship
- Service work
- Fellowship
- To anybody & everybody who wants it.
- This program is for those who want it, not those who need it!
- We ourselves are living proof of this.
- Therefore, the newcomer is the most important person in any meeting and in the program in general.
- Therefore, you must continue this hospitality!
- Practice these principles in all our affairs.
- We practice these daily, this is what we do.
- These principles are the 12-Step Program.
- In all our affairs.
- We don’t pick and choose.
- This is our new way of life.
- Likely much different from our former way of life!
Relapse; Meditations & Promises
- If we are casual with this phase of our development, we will be using before we are half-way through.
- We are going to know a new imprisonment and a new misery.
- We will relive the past and won’t be able to shut the door on it.
- We will comprehend the word CONFLICT and we will know PAIN.
- No matter how far down the scale we have gone, we’ll sink even lower.
- That feeling of uselessness and self-pity will deepen.
- We will gain interest in selfish things and lose interest in our fellows.
- Self-esteem will slip away.
- Our whole attitude and outlook upon life will SUCK.
- Fear of people, and of economic insecurity will multiply.
- We will intuitively know how to run from situations which never used to bother us.
- We will suddenly realize that God would never have done to us what we are doing to ourselves.
- Are these extravagant promises?
- We think not!
- They are being fulfilled among those of us who are still drinking; sometimes quickly, sometimes slowly…..
- IF WE USE FOR THEM!
- Are these extravagant promises?
Neuroanatomy & Brain Evolution
(Orientation: This is the brain, sliced in half, from top to bottom dividing right & left sides, this is the view of the “inside” of the right half of the brain.)
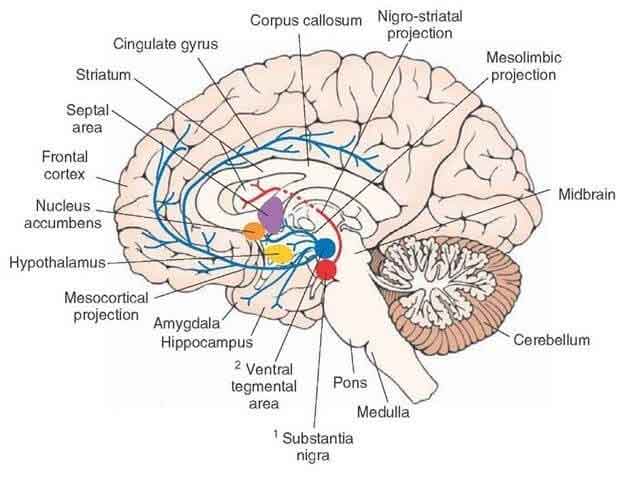
Addiction Anatomy
(Orientation: This is the brain, sliced in half, from top to bottom dividing right & left sides, this is the view of the “inside” of the right half of the brain.)
Neural Pathways Involved in Addiction
- New neural pathways form as addiction progresses
- They also form in withdrawal
- But those prior pathways are “circuits ready to be re-energized at a moment’s notice”
- Therefore, when folks relapse, they don’t start out their addictive disease at the level of when they first became addicted…
- They typically relapse to a degree of use that was greater than what they were using when they had most recently stopped using
- Even if it was decades ago!
- Those pesky neural circuits still exist
- Think of a superhighway that was built, used for awhile then for whatever reason falls into disuse—very little traffic but many available lanes available and able to carry a lot of traffic.
- Addiction changes brain structure and function
- Impaired decision making
- Impulsivity is controlled by the pre-frontal cortex, which changes in addiction.
- Compulsivity in the pre-frontal cortex changes in addiction leading to…
- Drug-seeking behaviors
- Cravings
- Habit formation
- Relapse triggers
- Stress dysregulation
- Withdrawal (with other more primitive brain areas)
- The pre-frontal cortex can be thought of as a “braking system” for impulsivity & compulsivity
- Addiction involves numerous structural changes in the brain such as the dopamine-2 allele in the locus ceruleus and other areas in those with addictive diseases.
- Mesolimbic system pathways are critical in the neurobiology ofaddiction:
- Located in the brainstem, the area essential for our basic survival.
- The Ventral Tegmental Area (VTA) is located at the front of the mesolimbic center.
- The VTA projects to the nucleus accumbens, the “reward center” of the brain.
- The main mesolimbic neurotransmitter is dopamine, the “feel good” neurotransmitter.
- Dopamine is released when we engage in activities that help further our survival and the survival of the human species (which involves sex!).
- This helps ensure our survival as a species; it makes us feel that good!
- ALL addictive drugs and activities release dopamine into the nucleus accumbens.
- Stimulant-type drugs release more than the other classes.
- Dopamine is associated with pleasure seeking and drug seeking/craving.
- GABA & Glutamate are also involved in pleasure-seeking.
- Dopamine is also involved in drug craving.
- Habituation; natural cravings (food, water, sex) lessen over time and with satiation.
- Dopamine activity decreases with habituation; once satisfied, enough is enough with “natural cravings”.
- Addiction is another matter; this is an unnatural desire.
- Tolerance happens as people need to increase the dose and frequency of their drug of choice to maintain the pleasurable effect/amount of dopamine which wears off after time and continued exposure to drugs.
- Tolerance leads to increased drug craving/compulsion to use
- This drives the addictive process forward
- As addiction progresses, cravings (compulsion) gradually replace pleasure seeking (impulsive), this is worsened with drugs such as opiates that have severe withdrawal symptoms in addition to craving.
- Craving is an attempt to avoid or relieve unpleasant symptoms.
- So, addiction starts with pleasure-seeking and ends up in the trap of using to relieve craving.
- Eventually the relief of craving becomes its own form of pleasure.
- As drug use or addictive activity escalates, the involvement of various brain regions associated with our emotional state also increases.
- The brain region most often associated with our emotional state is the extended amygdala, part of the limbic system (where our emotions “live”).
- Interestingly, the olfactory bulb is located right next to the amygdala.
- Scents/smells often have a strong impact on our emotional state for this reason.
- Scientists think this brain region plays an important role in addiction because of its association with emotions and stress.
- The brain region most often associated with our emotional state is the extended amygdala, part of the limbic system (where our emotions “live”).
- Dopamine is released when we engage in activities that help further our survival and the survival of the human species (which involves sex!).
- The amygdala processes emotions and memory.
- When the brain forms these memories, it stores the memory of the event along with the emotions that accompanied the memory.
- The memory of engaging in the addiction is stored with a pleasant emotional state (positive memory).
- Thus, the pleasing memories of engaging with an addiction can lead to repeating those behaviors and a habit forms.
- Emotional memory has another role in the development of addiction called due anticipation.
- Cue anticipation refers to environmental cues that can initiate or elevate cravings. Cravings often lead to relapse.
- For this reason, these cues are often called relapse triggers.
- These environmental cues (relapse triggers) can be anything that is associated with the addiction.
- The brain may also form an association between unpleasant emotions and a memory (forming a “bad” memory).
- The negative emotional memory of anxiety becomes associated with the physical signs of withdrawal.
- As withdrawal begins, the symptoms trigger an unpleasant emotional memory.
- This increases the negative experience of withdrawal.
- This acts as a “feed-forward) or amplification loop within the neural circuitry.
- Withdrawal avoidance (via returning to the addiction) often becomes the cornerstone of addiction in the later stages.
- Thus, in the earlier stages of addiction, the pleasurable experience of the drug motivates a repetition of that behavior (impulsive).
- In the later stages, (compulsive) relief of withdrawal symptoms (physical and/or emotional discomfort) achieves pleasure.
- The pleasurable relief from withdrawal symptoms continues to motivate the repetition of that behavior.
- Addiction is like dancing with an 800-pound gorilla.
- Exciting at first (impulsive).
- Then a habit that you do (compulsive).
- Addiction is like dancing with an 800-pound gorilla.
- Finally, you’re exhausted, but you’re not done dancing until the gorilla is done dancing!
- Stress and the role of the hypothalamus;
- The hypothalamus regulates body temperature, hunger, thirst, sleep and our response to stress.
- The hypothalamus signals the pituitary gland to release hormones (endocrine system) which affect distant parts of the body, not just within the brain as neurotransmitters do.
- Think of the “fight or flight” of the autonomic/sympathetic nervous system.
- These hormones can also act as neuromodulators within the brain, like a neurotransmitter acts.
- A medical intuitive, gifted with a sixth-sense regarding disease and healing refers to the hypothalamus as the “location of our soul”.
- The hypothalamus signals the pituitary gland to release hormones (endocrine system) which affect distant parts of the body, not just within the brain as neurotransmitters do.
- Stress is a major trigger for relapse
- Relapse is a bigger problem than withdrawal for addiction patients
- Stress and psychostimulants cross-react with each other, promoting relapse
- Psychostimulants (amphetamines, cocaine, methamphetamine) are more difficult to get off of than other addictive drugs due to this cross-reactivity at the neurotransmitter level.
- Withdrawal also causes stress.
- This creates an unfortunate cycle.
- Efforts to stop using create stress.
- Stress triggers release of stress hormones from the hypothalamus.
- Dopamine and serotonin activity in the nucleus accumbens actually decrease with stress early in recovery.
- These calming neurotransmitters normally help reduce stress.
- This is a disruption of the normal stress response that occurs with addiction & withdrawal.
- The hypothalamus regulates body temperature, hunger, thirst, sleep and our response to stress.
- The dopamine and serotonin neurotransmitters should increase to help cope with the stress.
- Stress triggers addictive behavior (use).
- Thus, withdrawal causes stress, which can trigger more addictive use, which causes stress to the addict who is unable to stop using the drugs in a vicious cycle in which the normal calming/“braking” serotonin/dopamine activity from the nucleus accumbens is lost!
- Recovery is the process of breaking this cycle.
- It takes a lot of motivation!
- Medication help, but recovery still requires effort!
- The brain is very adaptable; it learns!
- This is what the brain was designed to do—learn!
- Recovery is a process of learning!
- Learning involves forming new circuits/pathways in the brain.
- Many recovering addicts will testify that the first effort at recovery is much easier than recovery after numerous slips or relapses.
- The first is a gift.
- It’s progressively harder to recover after the first attempt.
- This is one of the spiritual axioms of recovery.
- Addiction related brain areas neurotransmitters and their functions;
- The negative emotional memory in the amygdala is associated with drug withdrawal.
- The positive emotional memory in the amygdala is associated with drug cues.
- Hypothalamic and nucleus accumbens serotonin (calming) & dopamine (feel good) disruption occurs due to stress de-regulation.
- The pleasurable relief from withdrawal symptoms that occurs by resuming drug use or addictive activities reduce stress/sooth the hypothalamus.
- Opioidsinhibit the firing of neurons in the locus ceruleus.
- Alcoholics & addicts have altered Dopamine-2 Alleles in the Locus ceruleus.
Comprehensive Overview of Addiction and the Process of Recovery
Comprehensive Overview of Addiction and the Process of Recovery
Slide Shows
Videos