
Comment; This protocol balances the Sympathetic & Parasympathetic Autonomic systems while improving nitric oxide production, normalizing cellular energy production, balancing other neurotransmitters, removing toxins and normalizing a variety of metabolic defects, promoting health.
Dr. Alan R. Vinitsky, M.D.
Sublingual or Intranasal B12 & Hydroxocobalamin Protocol
INTRODUCTION In Energy-the Essence of Environmental Health (Alan R. Vinitsky, M.D. and Natalie Golos, 2004, in press, authorhouse.com), the Accordion Reserve has been advanced as a model to represent optimal health. The size and movement of the Accordion is influenced by the Autonomic Nervous System (ANS) – proposed controller of all organ systems.
As the Accordion’s size diminishes,the SNS dominates. As the Accordion expands, PSNS governs. Maximal size and flexibility of the Accordion represents optimal health.
The keyboard of the accordion represents Environmental Factors (biologic, chemical and physical), and the buttons handle attached to the bellows represents Energy.
Energy Factors include sleep, exercise, nutrition and relationships (with one’s self, others, one’s external and internal environment – genes, cellular structures, organs and organ systems – and a spiritual or Guiding Force.) The goal of all scientists and healers in the health fields is to identify those treatments that fully restore health safely and economically. The Accordion Reserve model predicts that balancing the ANS is a necessary condition to restoring health. The hypotheses and treatments below evolved from that understanding.
NEUROTRANSMITTERS
The actions of nerves are dependent on chemical messengers called neurotransmitters. Some of these are: adrenaline, serotonin, dopamine and norepinephrine.
METHYLATION
The chemical reaction called methylation is crucial to the functions of life. More than eight major processes of methylation are dependent on two vitamins: folic acid and B12.
Critical to understanding the treatment utilizing folic acid and vitamin B12 in restoring health is the novel hypothesis that methylation pathways have a priority of functions within our bodies. If the hypothesis is tested and proven, then it follows that the body will attempt to protect the highest priority methylations at the expense of those lower on the list.
Based on observations of nature, the chemical reactions or functions below, all requiring methylation, are proposed in a tentative ranking order from highest to lowest:
1. activating adrenalin
2. inactivating adrenalin
3. inactivating histamine
4. inactivating serotonin, dopamine and norepinephrine; activating melatonin
5. inactivating chemicals that look like adrenalin (catechols, such as estradiol)
6. inactivating niacin
7. inactivating toxins, chemicals and medications
8. contributing to DNA, RNA and protein (enzyme) synthesis
9. activating creatine
The above ranking is based on the premise derived from the Accordion Reserve model that the body must first be alerted to stress. However, sustained activation of adrenaline is self-destructive and must be quickly terminated.
Recognizing the seasonality of diseases for some individuals (such as an increased incidence of gastric and psychiatric disorders in spring and fall), for them inactivating histamine is a high priority. The body must then recognizes the need to obtain proper sleep for healing; hence, the requirement for proper balance of serotonin, dopamine and norepinephrine.
Removing toxins and inactivating less important hormones would also be more protective. Healing and repair can proceed at a significant rate only if activities ranked higher are also maintained.
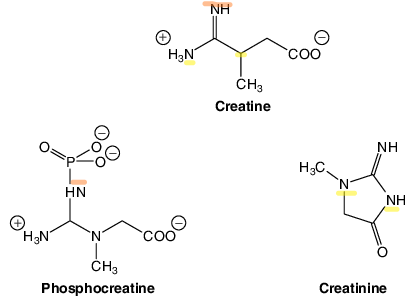
Finally, creatine production, other than that which is absolutely necessary for life’s basic muscle function, is inherently wasteful. Creatine is a storage molecule for energy in muscle. Muscle builders use it as a supplement to generate muscle mass and in urine. The methyl group that is necessary to create creatine is not recoverable. Failure to generate extra creatine may explain the observation that muscle mass declines 10% per decade of life after age 40.
The implication of the above ranking is that chemical reactions lower on the list are still proceeding, but perhaps with lesser activity. Or they may be temporarily or chronically sacrificed in times of stress or serious illness. Reverse thinking suggests that if optimal health is present, all functions in the above list will continue at the necessary level of function, performance and integration.
AUTONOMIC NERVOUS SYSTEM (ANS) DYSFUNCTION
Observations of chronic malfunction of the ANS suggest that as the Sympathetic Nervous System (SNS) gets stronger, the Parasympathetic Nervous System (PSNS) gets weaker over time, unable to compensate and normalize the SNS. Eventually, the SNS weakens as well, and neither branch can function successfully. This condition is a prelude to chronic illness and death. This feedback loop is at least likely to occur in the nucleus solitarius of the brainstem. The following hypothesis attempts to explain this phenomenon.
FORMALDEHYDE
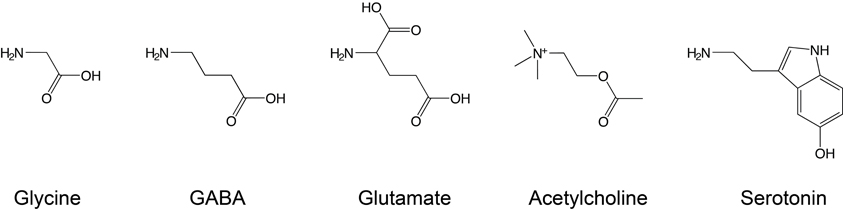
The PSNS is regulated by another neurotransmitter; Acetylcholine (ACh). The neurotransmitter is recycled for continuous functioning of the nerve. In this hypothesis, compensatory increase of PSNS is necessary to down regulate SNS activity. However, incomplete recycling of ACh may lead to its increased metabolism. Choline which has 3 methyl groups on a glycine skeleton, is the first byproduct. One methyl group then becomes formaldehyde.
Formaldehyde is a simple one carbon molecule, oxidized from methane via methanol. Formaldehyde can then be oxidized to formic acid. Inherently toxic, it is remarkable that the body actually generates formaldehyde. The concept, however, is no different from the body’s production of carbon monoxide.
Formaldehyde is known to cause increased sympathetic activity. If left uncorrected, this sequence can result in the vicious downward spiral of increased sympathetic activity.
MUSCLE FUNCTION
In the simplest expression of muscle contraction, the motor unit is regulated by a nerve that depends on Acetylcholine to fire. While this nerve function is not a part of the ANS, it nevertheless is potentially subject to the same metabolic dysregulation. Thus, excess formaldehyde production in muscles could increase sympathetic activity, reduce blood flow, reduce proper utilization of glucose for muscle energy and cause increased lactic acid production. The result would be increased insulin production, increased fat deposition, lower blood sugar, and so on. This would form the basis for the insulin resistance or metabolic syndrome precursor to diabetes.
FOLIC ACID
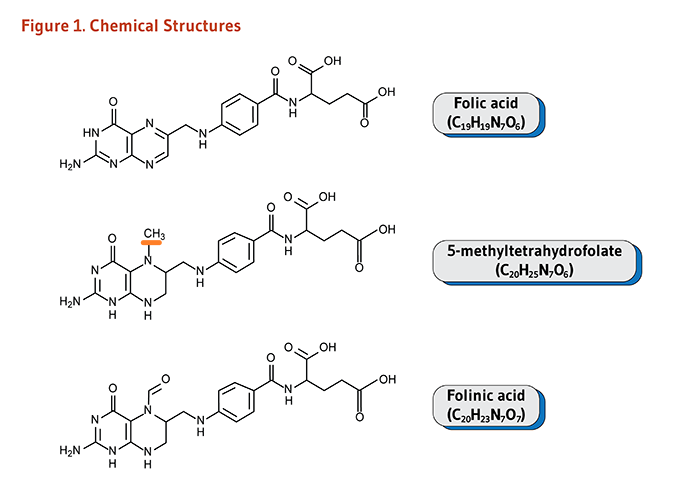
A large complex vitamin, folic acid has an almost obligatory affinity for formaldehyde. Perhaps it is this vitamin that is the ultimate protector of the human body. However, it is also known that too much folic acid is not good. By trapping all the formaldehyde(or methyl groups), proper building, repairing and healing cannot occur.
VITAMIN B12 (COBALAMIN)
Another large complex vitamin, cobalamin functions as the receiver for folic acid to deliver methyl groups to perform the functions listed under “Methylation” above.
COMBINED FOLIC ACID AND VITAMIN B12
The hypothesis for the“21st Century Miracle Treatment” is derived from understanding and observing that it is simply insufficient to supply oral supplementation of these two nutrients and expect people to recover. The reasons are as follows:
1. Folic acid is absorbed in the proximal small intestine (close to the stomach), while vitamin B12 is absorbed in the distal small intestine (near the large intestine).
2. Both vitamins are subject to interference’s of absorption, either by genetic defects, injury to the lining of the intestines, or direct blockade (such as ethanol’s effect on folic acid).
3. High blood levels of the vitamins are observed in persons who remain ill. If maximal methylation is to occur, so that all levels of priority can be accommodated, then maximally available folic acid and vitamin B12 must be available simultaneously to signal the enzymes to perform at the optimal rate. The best way to assure such immediate availability would be delivery by either the sublingual or the intranasal route. Other delivery systems such as lung inhalation, injection and transdermal are also possible. Of these, the transdermal route offers the possibility of prolonged delivery (corresponding to the sublingual-transdermal nitroglycerin comparison to treat angina pectoris.) A potential advantage of the intranasal route may be to by-pass the blood-brain barrier, so that both vitamins will enter brain tissue.
DOSAGES OF FOLIC ACID AND VITAMIN B12
Thus far, the sublingual route has been compared on a limited basis to the oral route and the following observations have been made:
1. Folic acid and vitamin B12 should be given in a ratio of about 5:2.
2. Doses may be given about every 3 hours.
3. Repeat or multiple doses may be given at shorter intervals, so long as the ratio is maintained.
FORMULATIONS OF FOLIC ACID AND VITAMIN B12
Folic acid comes in several forms. Technically, most folic acid is synthetic and is in an oxidized form. It requires an enzyme to activate (reduce) the vitamin for use in the methylation pathway. The form we have used comes as 5 mg/drop.
Vitamin B12 is also available in multiple forms. The most readily available is cyanocobalamin, but this form is not found in nature and is most likely useless in this treatment protocol. The preferred form is the oxidized hydroxocobalamin.
The active forms in the body are methylcobalamin (in the cytoplasm of cells) and denosylcobalamin (in mitochondria). An intermediate form called glutathionylcobalamin forms from the hydroxocobalamin in the cytoplasm. Methylcobalamin is also the dominant form in the plasma and is carried on a protein. Hydroxocobalamin is ordinarily taken up by a different protein or remains free in the plasma. It is the hydroxocobalamin that actually penetrates the cells, becomes reduced to glutathionylcobalamin prior to its conversion to active methyl- or adenosylcobalamin.
One drop of folic acid (5 mg/drop) is dripped on 1 tablet of 2 mg hydroxocobalamin. Together the vitamins are immediately placed under the tongue and held there until the tablet completely dissolves.
IMBALANCES OF FOLIC ACID AND VITAMIN B12
Observations of nature noted the following:
1. Taking both high doses of folic acid and vitamin B12 orally resulted in muscle cramping, “restless legs” and interrupted sleep. Recognizing that the vitamin B12 was taken orally(when it was supposed to have been taken sublingually) was corrected by taking the sublingual dose. Symptoms abated within minutes.
2. Taking a relatively low oral dose of folic acid and a high sublingual dose of vitamin B12 at different times resulted in an anxiety situation (other factors may also have played a role.) However, titration of oral folic acid over a half hour to a total dose of 5 mg resulted in temporary cessation of anxiety, high blood pressure and pulse. The effect wore off in 20 minutes and improved again with another 1 mg of folic acid.
3. Using other formulations of vitamin B12 had no substantial impact on improvement of the methylation pathways.
4. Using sublingual folic acid with sublingual vitamin B12 improved responses and clearance of symptoms.
EFFECTS OF COMBINED FOLIC ACID AND VITAMIN B12
Observations were made of patients who have tried high dose combined sublingual folic acid and vitamin B12. Previously these patients had been trying standard doses and regimens of folic acid and B12 without success.
1. Some autistic children have now responded more successfully to other remedies employed to help them heal other aspects of their condition.
2. A child with Rett’s Syndrome (a genetic condition of extreme sympathetic over-activity) is sleeping for the first time in her life.
3. Hyperactive children become calmer and more focused.
4. People with fatigue have started to gain more energy.
5. Individuals with Chemical Sensitivity have reduced symptoms to exposure. Their symptoms can sometimes be aborted with folic acid and vitamin B12 combined. They are able to distinguish what triggers are setting off their symptoms.
6. People with shortness of breath have resolved symptoms of what appeared to be asthma and were observed to improve their forced vital capacity on pulmonary function testing.
7. Anxious people have felt calmer.
8. Exercise tolerance and endurance have increased without increasing pain and injury.
9. Some people with chronic pain and acute injury pain have responded with pain relief more briskly than expected. Symptoms of neuropathy such as numbness, tingling, and balance disturbance are improved.
10. Healing of diabetic foot ulcer occurred more rapidly than expected.
11. Persons have been able to reduce their doses of pain and anxiety medications without the need of medications to reduce or block withdrawal symptoms.
12. Individual with Parkinson’s disease had reduced dyskinetic movements.
13. Person with memory dysfunction and “brain fog” had improvement in symptoms.
14. Patients with diabetes and cholesterol metabolic dysfunctions have noted improvements in their metabolic parameters.
15. Persons with blood pressure elevations and tachycardia noted a decreased requirement for medication, and their vital signs were improved.
16. People have reported improved sleep, decreased nocturia, urgency and frequency. Daytime sleepiness has diminished.
17. Some allergic individuals have noted fewer allergy symptoms.
NITRIC OXIDE
Another neurotransmitter that plays a vital role in nerve, muscle, gut and blood vessel function is nitric oxide. It is a short-lived molecule that cannot be stored. Its production is stimulated in central nervous system tissue by NMDA (N-methyl D-aspartate) receptors, which, in turn, are stimulated by glutamate.
FOLIC ACID AND NITRIC OXIDE
Recognizing that folic acid has a glutamate attached and that humans have an enzyme that adds more glutamate to it, high levels of brain folic acid may also scavenge for glutamate, just as it may for formaldehyde. If so, then, as folic acid collects extra glutamate, fewer NMDA receptors are stimulated. That effect may be to reduce seizures, pain, and any other function typically stimulated by glutamate. At the same time those extra polyglutamate folates do not participate in methylation. In the reverse, folic acid then serves as a reservoir to dispense glutamate to stimulate NMDA receptors. As the glutamate is liberated,folic acid participates in methylation. Similar relationships can be expected in the gastrointestinal tract, muscles, and other sites where folic acid and nitric oxide co-exist.
TOXINS AND METHYLATION
Mercury and other metals inhibit the function of the methylation enzymes. Aluminum and lead enhance mercury’s toxicity. Cadmium mimics mercury’s effect. Many of the toxic metals of exposure are methylated in the course of their metabolism, either activating (mercury) or inactivating them (arsenic.) Organic mercury (such as the immunization preservative thimerosal) is especially toxic.
HEALING AND THE AUTONOMIC NERVOUS SYSTEM (ANS)
The success of an individual to endure stress of either a physical or emotional nature is dependent on the flexibility and resiliency of the ANS. In the ideal, optimal state of health, that person should not only endure but also completely recover from the given cumulative stress. Failure to complete that complex function is tantamount to a declining Accordion Reserve. Thus,any individual who is being treated for a chronic disease condition has implied ANS dysfunction.
Another derivative of this understanding is that antecedent ANS dysfunction may be the precursor to developing further illness. Hence, ANS dysfunction may precede diabetes, hypertension and other conditions, rather than occurring in the reverse order.
Repair and healing are dependent on generating, storing and effectively utilizing energy for restoring tissues to their previous functions. In some instances, this concept may actually extend to repairing gene defects and mutations. While repair of inborn errors through methylation may still be a dream, it is expected that acquired defects exhibiting partial expression of a condition may be susceptible to repair. Perhaps the limitation will be: how efficiently can all the methylation pathways operate in an integrated pattern, once there is complete saturation of folic acid and vitamin B12?
Based on the model and hypotheses presented, when creatine production is increased, exercise performance will improve. Nitric oxide in muscle will be used to improve glucose transport rather than to generate inflammation. Results will be to reduce pain,
increase or sustain muscle mass, reverse insulin resistance and correct chronic disease patterns. Other genetic syndromes based on non-fixed or partial expressions mutations will have the potential to heal.
QUESTIONS CONCERNING HIGH DOSE FOLATE AND VITAMIN B12
Question 1: How many doses are needed each day? Is there a maximum dose? Can the dose be other than a 5:2 ratio of folic acid: vitamin B12? Are the doses different for children and adults?
Answer: Minimally 3 doses daily are required, otherwise there appears to be a wear-off effect, sometimes as soon as 3 hours. No maximum dose has been identified. Some people have taken 10 doses daily. The medical literature suggests that for a folic acid deficient malabsorption situation 100 mg of folic acid daily was required. It is possible that a different ratio may be necessary for other individuals. Initially, pediatric doses were initiated at a lower dose, but the ratio was maintained. Taking the two vitamins sublingually at the same time appears to limit side effects. Higher doses for children are now recommended. The limit on dosing appears to be dependent on the instability and rigidity of the ANS.
Question 2: Are there any adverse effects to combined high dose folic acid and vitamin B12-hydroxocobalamin?
Answer: Most individuals of all ages have tolerated these high doses very well. When vitamin B12 2 mg was given by itself or with minimal folic acid that was eventually adjusted upward toward 5 mg, symptoms of adrenaline production occurred; jitteriness, shaking, cold extremities, hunger, tachycardia, head rush and headache. These symptoms were usually of short duration. When enough folic acid was taken with vitamin B12 side effects were minimized. As repeated doses were taken, these adverse effects were also reduced. Symptoms were also noted when doses wore off, sometimes at approximately 3 hours. Relief returned with taking another combined dose. When high dose folic acid was taken without vitamin B12 or vitamin B12 was taken on a delayed basis, some individuals noted anxiety, muscle achiness, prolonged fatigue and impaired sleep. Symptoms occurred alone or in combination. A dose of vitamin B12 sublingually almost immediately corrected the symptoms.
Question 3: How long is treatment needed? What identifiers are used to indicate that treatment is working?
Answer: There is no indicator yet as to how much or how long treatment is to be continued. It is hypothesized that when serum creatine levels begin to rise, then methylation enzyme pathways are beginning to work in muscle. That marker may suggest that functional levels of the vitamins are approaching normal. These finding should also correlate with noted improvements of parameters in other organ systems that are being treated by any other protocol.
Question 4: What other observations have been noted with combined folic acid and vitamin B12 therapy?
Answer: Protocols for conditions often involve side effects or adverse reactions. Scan the Physicians Desk Reference and note that symptoms of opposite extremes are listed for the same medications. Most likely, those represent the Autonomic Nervous System reacting adversely. By stabilizing the ANS, side effects from usual treatments for other conditions will be more likely tolerated.

- COVID UPDATE: What is the truth? - 2022-11-08
- Pathologist Speaks Out About COVID Jab Effects - 2022-07-04
- A Massive Spike in Disability is Most Likely Due to a Wave of Vaccine Injuries - 2022-06-30
