
Comment; Excellent review by the director of Great Plains Laboratory on the toxicity and metabolism of oxalates
MARCH 26, 2010 BY WILLIAM SHAW55 COMMENTS
Read this in: Nederlands

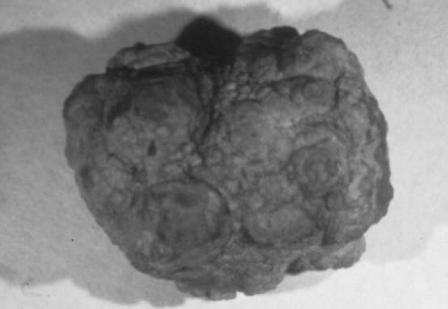
A mummy that had been preserved for a couple of thousand years in the high desert of Chile was discovered upon X-ray examination to have a very large oxalate stone in the kidney, about the size of a golf ball. The discovery of this ancient sufferer is testimony to the fact that kidney stones and oxalate toxicity have afflicted humans for a very long time.
Oxalates (the salt form of oxalic acid) are extremely painful when deposited in the body. About eighty percent of kidney stones are caused by oxalates and they are by far the most common factor in kidney stone formation. There is also a large degree of genetic variability in the ability to detoxify the chemicals that produce oxalates. Perhaps twenty percent of the population has a genetic variance that increases their likelihood of producing oxalates, even when not consuming a high-oxalate diet.
STONED
Oxalates can form all throughout the kidney and the urinary tract, and can also form in the ureter as well as in the bladder. These star-shaped crystalline stones cause pain as the pressure in the urinary filtrate builds up, and perhaps also by tearing into the walls of the urinary tract itself.
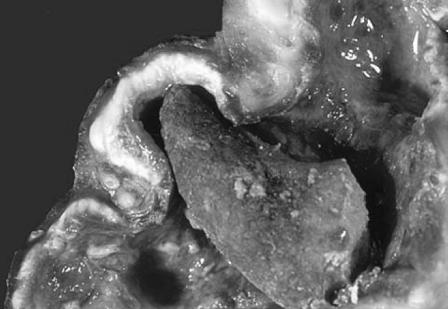
Some kidney stones acquire a stag horn shape, while some oxalate crystals resemble pieces of coral. The crystals do have a lot of calcium in them just as coral does. Oxalate crystals appear in different colors. Some are black and almost look the color of Indian arrowheads made of obsidian. On page 41 is shown a picture of a kidney with one of the oxalate crystals imbedded in it. You can see that the crystal is very pointed. Some of these have extremely sharp ends that cause severe pain.
Kidney stones are one of the most common medical ailments—ten to fifteen percent of adults will be diagnosed with a kidney stone in their lifetime. One million Americans develop kidney stones each year and most of these are oxalate related. Seventy-five to ninety percent of kidney stones are made of oxalic acid bound to another compound, usually calcium.
Once you have experienced a kidney stone attack, you have a very high chance of having another unless you change your way. The common symptoms are pain in the side and the back below the ribs. The episodes of pain last between twenty to sixty minutes, and it is common to hear women who have suffered kidney stones claim that they are more painful than childbirth.
The pain radiates from the side and the back to the lower abdomen and groin. There may be bloody, cloudy and foul-smelling urine. If there is infection, there may also be fever and chills. Pain with urination may accompany nausea and vomiting, and the sufferer may have a persistent urge to urinate.
This last symptom is a common factor in autism. It has been noted that many children with autism urinate perhaps fifty times a day, but only release a small amount of urine each time. After I did my research it became clear that the behavior arose because these children were suffering from kidney stones and high oxalate concentrations. The children would urinate only a small amount at a time since when urinating normally the pressure of the stream causes pain. Frequently releasing small amounts of urine causes much less pain to the child.
NOT JUST IN THE KIDNEYS
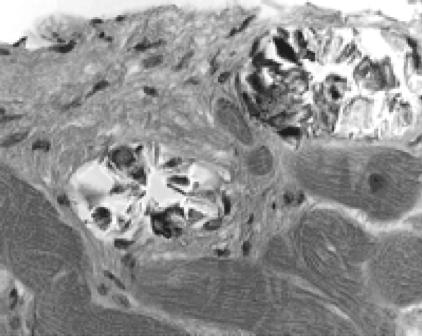
Even though oxalate crystals are most common in the kidney, they also can form in virtually any other tissue in the body, including the brain and the blood-brain barrier. Oxalate crystals resembling pieces of glass can form in the heart muscle. As the heart muscle contracts, these pieces of oxalate crystals actually tear into the tissue. If these crystals are deposited in skeletal muscle, normal movement and exercise can be very painful. I’m convinced this is also one of the factors responsible for fibromyalgia. Oxalates may also cause thyroid disease as they react in thyroid tissue.


Oxalate crystals can form in the bone. The oxalate crystals can become so dense they actually push the bone marrow cells out of the bones, leading to severe anemia. Deficiencies of red blood cells as well as white blood cells may result due to the oxalate depositions in the bones. Oxalates can likewise cause osteoporosis. The oxalates form in the bone marrow and alter the structure of the bone matrix so the bone is much weaker and prone to breakage.
Other diseases in which oxalates may play a role include arthritis, joint pain and interstitial cystitis.
PROPERTIES OF OXALATES
The shape of the crystal will depend on which metal the oxalate combines with. Calcium is one of the most common but it can combine with virtually any metal. There are cobalt oxalates and zinc oxalates. The cobalt ones are spear shaped whereas the zinc oxalate resembles thin disks. These are extremely thin and very sharp.
Oxalates in the gastrointestinal tract have a tendency to bind essential elements. If you have a lot of oxalates, you won’t be able to utilize essential elements like calcium, magnesium and zinc because they will also form deposits with oxalates. If you have excess oxalates, you may have to increase your intake of calcium, magnesium and zinc. In addition, rather than acting as antioxidants, oxalates are prooxidants, so they encourage the oxidation of your fats, forming rancid fats in your body.
A FUNGAL ORIGIN
An unexpected finding is the fact that oxalate crystals are produced in very high amounts by molds and fungus. Aspergillus—a common organism that causes infection in humans and also is found in the black fungi that you see in your bathroom—produces oxalates.
I remember I was in San Juan, Puerto Rico, at the old fort that overlooks the sea. There was a lot of black mold on the walls and I could see stalactites coming down. The stalactites in this case were formed from calcium oxalate. Aspergillus produces these oxalates, and these stones will form any place that has infection by the fungus.
In the case of sinus infection, mold and fungus, not bacteria, are the most common causes of infection. A colleague of mine, who is an eye, nose and throat specialist, X-rayed a patient’s sinuses and found large oxalate crystals in her sinuses, which disappeared after anti-fungal treatment.
Large oxalate crystals have also been isolated from the lungs of people who had Aspergillus infection of the lungs. The deposits can also form in the skin where they create black areas and necrotic lesions in people with very high oxalate levels.
OXALATES AND AUTISM
I first became interested in this topic because of improvements that were noted in autistic children by the researcher Susan Owens. It was Owens who collected the data showing that many autistic children had frequent urination of small volume and found that the phenomenon was associated with oxalates. She also found that these children often manifested gastro-intestinal symptoms such as diarrhea and stomach pain. They may also have pain in the urinary tract. That pain is relieved when a low oxalate diet is instituted. Owens also found that children had improved cognitive, academic and motor skills once the amount of oxalates in their diets was sharply reduced. The same dietary measures helped reduce pain in their muscles and feet, and also brought about a reduction in abnormal behavior and self-abuse as well.
Eighty percent of people with genetic diseases that cause them to produce kidney stones die before the age of twenty. These genetic diseases, which belong to a class of disorders called hyperoxaluria, are frequently fatal unless the victim receives both a liver and a kidney transplant. Sometimes even after the transplants people die because the oxalates are deposited in tissues all throughout the body. The oxalates will come out of the bones or the muscles and then form in the transplanted kidneys and still kill the person.
More than a third of children with autism have oxalate values as high as people who have these rare genetic disorders, even though these autistic children do not have the disorders. The question naturally arose: If they don’t have this genetic disorder, why are their oxalates so high?
We correlated the amount of oxalate in autistic children with other biochemical parameters and found there was a high correlation with the sugar arabinose, which is a Candida marker. It appears that the main reason for the high oxalates in children with autism is because of the Candida problem, which is prevalent in autism. Arabinose is very low in normal children and very high in those with autism. We found in my earliest research that treatment with the anti-fungal drug Nystatin markedly decreased this compound. In addition, autistic symptoms such as hyperactivity, lack of eye contact, and aggressive behavior markedly decreased as well. Because of the dramatic reduction in symptoms, anti-fungal treatment has become one of the most common therapies in autism in the world today.
VULVODYNIA
Another condition associated with oxalates is vulvodynia, or pain in and outside the vagina. The oxalate crystals act like tiny pieces of glass, which are deposited in the tissue. The oxalate is extremely acidic so it is corrosive as well. The pain is often described as burning or stinging, with a feeling of rawness or irritation.
One of the published studies on the treatment of this condition states that this is due to a reaction with yeast. There is indeed a connection of vulvodynia with yeast, most often Candida. There are about a dozen different species of Candida yeast normally associated with humans, the most common of which is Candida albicans. It was found that the main way to treat volvodynia was anti-fungal treatment to get rid of Candida, along with a low-oxalate diet. These two approaches have been very effective in correcting this condition.
Children who take oral antibiotics will frequently have much higher amount of oxalates. Antibiotics severely disrupt the balance of normal flora in the gut, with a consequent exponential proliferation in the growth of Candida, which is resistant to antibiotics. Oral antibiotics first appeared in the early 1950s, and the pharmaceutical companies actually included antifungal drugs along with the antibiotics because they knew about this problem. The FDA disallowed the addition, declaring that there was no approval for the prophylactic use of anti-fungals, thereby washing their hands of the whole business. It is significant to note that if individuals are given the same amount of antibiotics intravenously, their oxalate values do not rise because there was no effect on the GI tract. In some ways the old medical treatment—a shot of penicillin—was a lot safer.
CHRONIC FATIGUE AND FIBROMYALGIA
Yeast is a common factor in chronic fatigue and fibromyalgia, and antifungal therapy is very useful in treating these problems. Jacob Teitelbaum has written several books about the treatment of fibromyalgia and indicates two-thirds of individuals improved their chronic fatigue and fibromyalgia after anti-fungal therapy.
A Dr. Eaton in England found that individuals who had chronic fatigue would actually produce alcohol from their sugar intake. He describes patients who would do a baseline blood-alcohol test, then take some glucose dissolved in a flavored drink, and measure the blood alcohol one or two hours later. The blood alcohol would be substantially higher if the person had a severe Candida problem.
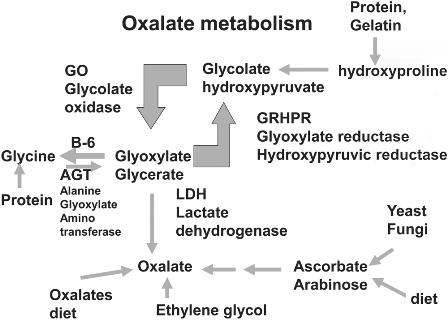
The OH component readily attaches to minerals like calcium, zinc and mercury, forming oxalates. Oxalates in the body come from food, can be formed in the gut by yeasts and fungi, or can result from an interruption in the glycolate pathway. Nutritional deficiencies and inborn errors of metabolism cause the formation of oxalates rather than the protein glycine.
Eaton found that by using this test he could monitor patients undergoing different treatments for chronic fatigue and fibromyalgia and found that 42 percent of patients improved just with sugar restriction alone. If he combined a low-sugar diet together with anti-fungal drugs, he had about a 78 percent success rate.
The most comprehensive study was that of a Dr. Jessop in California, who treated over one thousand people with chronic fatigue and fibromyalgia using a single anti-fungal drug, ketoconazole. Eighty-four percent of the patients improved. Of the 1,100 patients, 685 were on disability payments. After the treatment with anti-fungal treatment, only twelve remained on disability. It was an extremely effective treatment!
ZELLWEGER SYNDROME
High amounts of oxalates have also been found in persons with a metabolic disorder called Zellweger syndrome, which causes the reduction or absence of an intracellular organelle called peroxisome, leading to mental retardation and severe metabolic problems. In one study, nineteen of twenty-three patients exhibited high amounts of oxalate, and there was a direct relationship between the degree of mental impairment in children and their levels of oxalates. The children with the highest amounts of oxalates were the ones who were the most mentally impaired.
OXALATES AND CANCER TREATMENT
Oxalates also come into play in cancer treatment. One of the drugs used to treat cancer, oxaliplatin, contains a combination of platinum and oxalate. In many of the people taking this drug, their cancer improved, but they also experienced severe neurotoxicity and nerve damage. While undergoing treatment, patients developed high amounts of oxalates which were coming from the drugs. Researchers found the effect was specific to the oxalates. If they gave the drug without the oxalate the toxicity did not occur; the toxicity was a result of the oxalate combined with the drug.
Research has also found that people with genetic variations called polymorphisms experienced much more neurotoxicity when exposed to this drug. Alanine-glyoxylate aminotransferase (AGXT) is the enzyme responsible for moderating the production of oxalates in the body. People with a genetic variation that leaves them deficient in AGXT are much more likely to suffer severe reactions. They suffer peripheral neuropathy, the disease of the peripheral nerves that causes superficial and deep sensory loss; sensory ataxia, which means not feeling a sense of balance; and functional impairment.
OXALATES IN FOOD
People who are vegetarians really have to be aware of all the oxalates they take in. The biggest culprit for all vegetarians is soy protein, and the second is spinach. Virtually everybody who eats a large spinach salad every day is going to succumb to kidney stones. I’ve tested them over and over again and the people who have the highest oxalate values invariably tell me that a cornerstone of their daily diet is a large spinach salad. If they add nuts to their salad and textured soy protein, both of which are very high in oxalates, you’ve got a cocktail made to produce kidney stones. Spinach is so high I would not recommend eating it even cooked, as a main course. Lettuces, by the way, are very low in oxalates. The biggest problem vegetarians face is eating a diet high in soy protein and spinach.
Once after I gave a talk a physician came up afterwards and told me that a few months earlier he had decided to get healthy. He decided to forswear all the McDonald’s and the like. He was going to start eating healthy and eating healthy meant a very large spinach salad with lots of pecans on it every day. Within two months he had kidney stones.
Cooking does not destroy the oxalates; they are extremely stable. Cooking may reduce the oxalates in foods as they precipitate into the cooking water, and if you discard that water you are likely reducing the oxalates remaining in the food. If you drink that pot liquor, however, you will absorb the full amount.
Peppercorns are very high in oxalates, but not many people eat a pound of black pepper every day. However, if you like pepper-coated steaks, pepper may contribute to your oxalate load. The same goes for parsley, it’s very high in oxalates but you don’t eat very much of it.
Peanuts and peanut butter are problematic because some kids eat them every single day. Peanut butter is not a poison, so eating it occasionally isn’t going to bother you. The problems come when you make a few highoxalate foods the staples in your diet.
Dr. Massey at Washington State University found that textured soy protein is very high in oxalates. There are 638 milligrams of oxalate per 85-gram serving, which is about the size of one of these small soy burgers and as much as you would find in a typical serving of spinach. The recommended amount of oxalate for people who have kidney stones is less than 30 mg a day. One soy burger contains twenty times the recommended daily dose in just one single portion. This, I would say, is a major problem for the soy producers. The soy cheese does not have nearly as much. It’s the textured soy protein, the soy burgers, the soy bacon that have such high levels. Some soy companies recommend that you pour textured soy protein on your breakfast cereal. You really don’t want to do that.
How much oxalate is in the typical diet? There’s a very large range— from 97 to 930 mg a day. To reduce kidney stones you should consume less than 30 to 50 mg a day.
TREATMENT
Even though we can avoid the worst offenders—soy foods and spinach— if you are enjoying a varied diet, it is difficult to reduce dietary oxalate levels to near zero because they occur in so many foods—grains, nuts, vegetables and fruits.
The most effective way to get rid of oxalates is the use of calcium citrate. This supplement exerts a double potency action in eliminating oxalate. The calcium part of calcium citrate binds to the oxalate and causes it to precipitate out in the stool so it will not be absorbed. But part of the oxalate escapes. The citrate is a second line of defense, which competes directly with the oxalate for absorption.
For the treatment to be effective, the calcium citrate must be taken at the same time as the oxalate-containing food. If you have problems with any of conditions caused by oxalates—kidney stones, autism or vulvodynia— then taking calcium citrate with each meal can be very effective. If there is an adequate amount of calcium in the diet—if supplementing with calcium citrate, for example—it will combine with the oxalate in the GI tract, precipitate out in the stool, and then be eliminated in the stool.
The optimum dosage is approximately 300-350 mg calcium as calcium citrate for a total of 1000 mg (one gram) of calcium a day. If you’re taking this you don’t need additional sources of calcium. An even better approach would be to use magnesium citrate. The adult dosage is about 300-400 mg a day. Some practitioners recommend up to 1000 mg but many people report problems with diarrhea if they exceed 400 mg. Again, a divided dose would be best, taking the magnesium citrate with each meal.
Some other supplements that can be very useful include probiotics and anti-fungal medication to help to control Candida. The probiotic bacteria have enzymes that break down oxalates.
The amino acid arginine helps to prevent the depositing of oxalates in the tissues. The omega-3 fatty acids and cod liver oil are also very effective in preventing oxalate deposition. The omega-6 fatty acids, mostly from commercial vegetable oils, behave in the reverse, and accelerate the deposition of oxalate.
The supplement that is most helpful is vitamin B6. This costs only pennies a day and is extremely safe. I take 100 mg every single day. I recommend just the pyridoxine form. I know the type called P5P is also used but personally I don’t think you get the additional benefit by the P5P.
There are a number of medical tests for oxalate status that we use at Great Plains Laboratory. We have a urine panel to measure oxalates and we can also test for yeast markers. We typically find that where the yeast marker is very high, the oxalate marker is also very high. We also test for vitamin B6.
With these measures, kidney stones are largely preventable. This is good news because oxalate buildup can do a lot of damage.
SIDEBARS
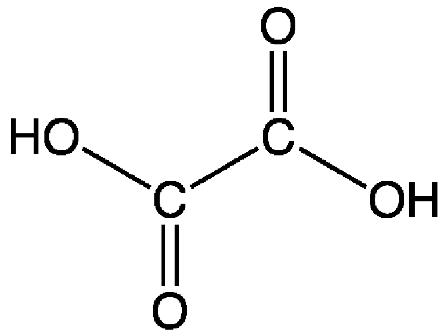
THE CHEMISTRY OF OXALATES
Oxalate refers to the salt form of oxalic acid. All acids follow the same convention of nomenclature. The salt of citric acid is citrate, for example. The salt form simply means it is missing hydrogen atoms. Instead, the salt form has a negative charge attached to it. When the acid has the hydrogen attached to it, it has the suffix –ic. When the hydrogen atoms are removed so that it is negatively charged, it has the suffix –ate. The critical thing about this, from the chemist’s point of view, is that the pH, which is a measure of the acidity of the molecule, of oxalates is the lowest of all the organic acids. (A low pH rating corresponds to a high level of acidity.) It’s the most acidic, most corrosive organic acid there is because of its very low pH value. For example, citric acid might have a pH of 5—mildly acidic in comparison, and hundreds of times less acidic than oxalate. The molecule of oxalic acid could lose two hydrogen atoms so it can become doubly negatively charged and this is the form in which oxalate is predominantly found in the blood and the urine. This form in which there are two negative charges makes it much more likely to bind to a number of metals. Calcium, zinc and mercury are examples.
What is very interesting from the chemist’s point of view is the fact that oxalate binds most tightly to toxic metals such as mercury and lead. One might think this strong chelating action is beneficial, but it is quite the opposite. Once oxalate binds with mercury or lead it immediately becomes insoluble and precipitates out of the bloodstream and forms crystals in the bones and other tissues. Rather than attaching to these toxic metals and escorting them out of the body, the oxalate traps the toxic metals within the body. This is one aspect of oxalates that I believe should be more closely examined as it may explain why oxalates are associated with so many diseases. They will trap heavy metals and enhance their toxicity.
The oxalate itself is water soluble, but once it binds with a metal ion it becomes insoluble and then precipitates out to be deposited in tissue. In a comparison of the different strengths of reaction of oxalates with various metals, the metal with the highest reactivity is mercury. When oxalate reacts with mercury, even if there is only a tiny amount present, it will preferentially bind with mercury compared to calcium or other metals. The oxalate almost seems to seek out and trap toxic metals. The reactivity of oxalate with calcium and magnesium, on the other hand, is very low, and the lowest reactivity is with magnesium. One of the treatments to help people get rid of excess oxalates is to take very high doses of magnesium, or in some cases, actually give intravenous infusions of magnesium. Because it has the least solubility with oxalates magnesium will help to dissolve them, so to speak.
OXALATE PATHWAYS
About fifty percent of oxalate comes from the diet and the other fifty percent comes from what your body makes itself. Oxalic acid in the diet is first converted to glycolate, then glyoxylate, and then at this point glyoxylate can either bind to a mineral to form oxalate or it can be transferred and form glycine.
If you have a genetic deficiency in the enzyme AGXT, the glyoxylate primarily forms oxalate because reduced amounts of AGXT do not function adequately to override this process. One in five people in the population has this genetic variant in which they cannot detoxify this compound. Instead it predominantly forms oxalate.
It has been found that one third of the people with oxalate toxicity have this genetic variant, and 53 percent of them are likely to have acute, very severe neurotoxicity versus only 4 percent in those with normal genotype expression. Probably a high percentage of people who have kidney stones are in this group of 20 percent of individuals with this genetic variant.
One of the body’s energy production factories called glycolysis is inhibited by oxalates. The enzyme pyruvate kinase is involved in the last step in the body’s energy production and is strongly inhibited by oxalate. It is very interesting that the same enzyme inhibition is largely responsible for Tourette syndrome. People with Tourette syndrome, however, have strep antibodies that inhibit this enzyme. Oxalates also strongly inhibit the same enzyme.
The critical factor here is that this enzyme works much better in the presence of high amounts of vitamin B6. This is another one of the holistic treatments for people with kidney stones. In fact, vitamin B6 treatment is also used by the mainstream medical community for people with kidney stones.
VITAMIN C, COPPER AND OXALATES
What about the controversy surrounding vitamin C therapy? Vitamin C has been shown to be very helpful in kids with autism, although theoretically vitamin C can form oxalates. I say theoretically. Vitamin C can increase your risk of kidney stones if you take extremely high doses, in the range of 100 grams (100,000 mg) a day.
A double-blind study found that very high doses of vitamin C was very effective in reducing autistic symptoms. A study showed that a person taking 2000 mg (2 grams) of vitamin C a day for ninety days did not cause a significant effect or change in oxalate levels.
Another study evaluated forty-five thousand men who took vitamin C and vitamin B6 over six years and examined the effect this supplementation had on their kidneys. In the six years of follow up they found 751 cases of kidney stones out of 45,000 men. There was no association, however, of vitamin C or vitamin B6 intake with the kidney stones. In fact, men who took more vitamin C had less risk of kidney stones than men who took less than 250 mg vitamin C.
The real problem with vitamin C is the metals that the person may be taking. If one is taking high amounts of copper or iron, these can accelerate the breakdown of vitamin C to form oxalates. Someone with high copper or iron levels may be at risk for higher oxalate formation if also supplementing with vitamin C. The vitamin C may be broken down to form dehydroascorbate and then oxalate. Knowing your copper and iron status can be very important.
If, for example, you have copper pipes in your home, which is very common, and you have acidic water, that water will dissolve your copper pipes so that most of the water coming out of your faucet will contain high amounts of copper. In turn, the high copper may cause you to degrade your vitamin C. There is a problem with forming extra oxalates, but this also means that even if you take high doses of vitamin C, it may not be useful because the copper can degrade it so rapidly. It is the free copper that is so toxic.
Copper is bound to a protein in the blood called ceruloplasmin. Isolating ceruloplasmin from blood was one of the first things I did after earning my PhD. I went to the Red Cross and obtained outdated plasma and I didn’t even have to test it. All I had to do was look at the color of the plasma. Donors who had high copper had serum that was green. I could pick out the samples with high copper just by looking at them in the freezer and choosing the green color.
Almost invariably the samples were from women who were on birth control pills. The estrogen causes the body to make more of this protein. We test this copper-zinc profile in the Great Plains Laboratory and the most important value is the free copper. A person with autism can have ten times the value of free copper compared to normal individuals. In some individuals with autism this can be most significant; but this copper-zinc imbalance is important in almost every chronic disease: ADD, schizophrenia, arthritis, chronic fatigue, and many others. When you have too much copper and not enough zinc, vitamin C will not be utilized, it will be destroyed.
SUPER HIGH OXALATE FOODS
| Spinach | Lime peel | Chocolate |
| Soy protein | Rhubarb | Instant coffee |
| Tofu | Swiss chard | Leeks |
| Peanuts | Parsley | Tea |
| Peanut butter | Sweet potatoes | Okra |
| Pecans | Pokeweed | Wheat germ |
| Lemon peel | Black pepper |
This article appeared in Wise Traditions in Food, Farming and the Healing Arts, the quarterly journal of the Weston A. Price Foundation, Spring 2010.

- COVID UPDATE: What is the truth? - 2022-11-08
- Pathologist Speaks Out About COVID Jab Effects - 2022-07-04
- A Massive Spike in Disability is Most Likely Due to a Wave of Vaccine Injuries - 2022-06-30
